
Recommended
More Related Content
Similar to 1-A-Hypersensitivity (general).pdf IMPORTANT
Similar to 1-A-Hypersensitivity (general).pdf IMPORTANT (20)
Recently uploaded
Recently uploaded (20)
1-A-Hypersensitivity (general).pdf IMPORTANT
- 2. • Hypersensitivity can be defined as an exaggerated response of the immune system leading to host tissue damage
- 3. Plasma cells • Plasma cells develop from B lymphocytes (B cells), a type of white blood cell that is made in the bone marrow. • Normally, when bacteria or viruses enter the body, some of the B cells will change into plasma cells. • The plasma cells make antibodies to fight bacteria and viruses, to stop infection and disease. Enlarge
- 6. T-cells • T cells express a receptor with the potential to recognize diverse antigens from pathogens, tumors, and the environment, and also maintain immunological memory and self- tolerance. • T cells are also implicated as major drivers of many inflammatory and autoimmune diseases.
- 8. Gell and Coombs’ classification scheme • On the basis of the highly influential Gell and Coombs’ classification scheme, there are four categories of hypersensitivity. – Type I— immediate hypersensitivity – Type II hypersensitivity - antibody-mediated cytotoxicity. – Type III hypersensitivity— complex-mediated – Type IV hypersensitivity— cell-mediated.
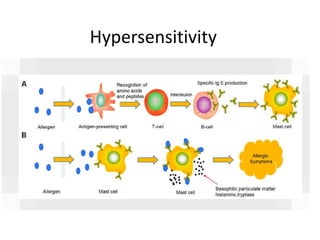
- 9. Type I— immediate hypersensitivity • anaphylactic or acute hypersensitivity • IgE antibody • mediated via degranulation of mast cells leading to release of preformed factors • promoting an influx of immune cells to the site of mast cell activation and initiation of a rapid inflammatory reaction.
- 10. • In the extreme case the inflammatory response extends beyond the localized site of initiation and affects systemic tissues leading to life-threatening anaphylactic reactions • Ex. Hay fever
- 12. Type II hypersensitivity - antibody- mediated cytotoxicity • caused by antibodies that are directed against cell surface antigens • IgG and IgM are the key antibodies
- 13. • cytotoxic events would include activation of the classical complement pathway leading to: – formation of a MAC – the attraction and activation of killing cells such as NK cells or phagocytes • Ex. blood transfusion reactions arising from mismatch of the blood ABO antigens
- 14. Type III hypersensitivity— complex- mediated • formation of large antigen–antibody complexes that circulate in the blood • coated by complement proteins • Removed by phagocytosis – If this process is compromised for any reason then the antigen–antibody complexes will be deposited in tissue capillary beds
- 15. • This deposition of high molecular weight antigen–antibody complexes in the glomerular capillaries of the kidney can lead to a condition termed glomerulonephritis which involves disruption of the glomerular basement membrane, destruction of glomeruli and ultimately renal failure which may necessitate organ transplantation.
- 16. • Systemic lupus erythematosus is a condition where autoantibodies are directed against the host’s DNA and RNA with subsequent complement-coated immune complexes deposited throughout systemic tissues such as in the kidney, skin, joints and brain.
- 18. Type IV hypersensitivity— cell- mediated • inappropriate accumulation of macrophages at a localized site • may or may not involve the presence of antigen. • Under conditions of ongoing localized infection or inflammation, macrophages release proteases, which destroy infected or otherwise damaged tissue
- 19. • However, with the inappropriate recruitment and/or activation of excessive numbers of macrophages, continuing damage to normal tissue may result, leading to chronic inflammation. • The recruitment and activation of macrophages in type IV hypersensitivity is augmented by the activity of helper T lymphocytes • Ex. contact dermatitis