cervical cerclage.pptx
•Download as PPTX, PDF•
0 likes•427 views

At the end of presentation, the participants should be able to understand the following: Definition of Cerclage Types of cerclage Indications Pre operative Preparations Removal of Cerclage

Recommended
More Related Content
What's hot
What's hot (20)
Similar to cervical cerclage.pptx
Similar to cervical cerclage.pptx (20)
More from Dr. Rahul Shah
More from Dr. Rahul Shah (6)
Recently uploaded
Recently uploaded (20)
cervical cerclage.pptx
- 1. CERVICAL CERCLAGE MODERATOR: Dr. Rehana Mushtaq PRESENTER: Dr. Rahul Shah PGY1 Department of Obstetrics & Gynaecology 1/9/2024
- 2. OBJECTIVE • At the end of presentation, the participants should be able to understand the following: • Definition of Cerclage and Types • Types of cerclage • Indications • Pre operative Preparations • Removal of Cerclage 1/9/2024
- 3. CERVIVAL CERCLAGE Provide structural support to “weak” cervix. Maintain cervical length and the endocervical mucus plug as a mechanical barrier to ascending infection. 1/9/2024 Principle: The procedure reinforces the weak cervix by a nonabsorbable tape, placed around the cervix at the level of internal os.
- 4. • Cerclage remains one of the standard options for prophylactic intervention in the care of women at risk of pretermbirth and second trimester fetal loss and is used by most obstetricians, despite difficulties in identifying the population of women who would most benefit. • The procedure, a stitch inserted into the cervix, was first performed n 1902 in women with a history of second trimester loss or spontaneous preterm birth suggestive of cervical insufficiency, with the aim of preventing recurrent loss. 1/9/2024
- 5. Types of Cerclage • History Indicated cerclage • Ultrasound Indicated Cerclage • Cervical Cerclage in increased risk cases of preterm delivery • Transabdominal cerclage • Rescue Cerclage 1/9/2024
- 6. HISTORY INDICATED CERCLAGE • Prophylactic in asymptomatic women • Elective in 12-14 WOG • Indications: >2 previous preterm birth and/or second trimester losses 1/9/2024 Not helpful in the decision for a history indicated cerclage. • Painless dilatation of the cervix. • Rupture of the membrane before the onset of contraction. • Cervical surgery. • Pre-pregnancy diagnostics tests: Cervical resistance Index, hysterography or insertion of cervical dilators.
- 7. ULTRASOUND INDICATED CERCLAGE • Indication: Previous one or more spontaneous mid-trimester loss or preterm birth and cervix is 25mm or less before 24 wog • Not recommended for funneling of the cervix in the absence of cervical shortening • Not indicated in women who have an incidentally identified cervix of 25mm or less with no history of spontaneous mid- trimester loss or preterm birth. 1/9/2024
- 8. Serial surveillance? +- USG indicated cerclage • Women with one or more second trimester loss or pre term delivery • Those who experience cervical shortening are at an increased risk of subsequent second trimester loss/preterm birth may benefit from US indicated cerclage. • Those whose cervix remain long have a low risk of 2nd trimester loss/premature delivery • Because the majority of women with a history of second trimester loss/preterm delivery will deliver after 33 WOG, no evidence to support serial sonographic surveillance over expectant management. 1/9/2024
- 9. Transabdominal Cerclage •Indications: Previous failed Transvaginal Cerclage •Associated with increased Maternal Morbidity •Can be performed before or in early Pregnancy 1/9/2024
- 10. Rescue Cerclage • Even with rescue cerclage the risk of sever preterm delivery and neonatal mortality and morbidity remain high. • Delay delivery by 5 weeks on average compared with expectant management (bed rest) alone • A/W 2 fold reduction in the chance of delivery before 34 weeks of gestation. 1/9/2024 Advanced dilatation of the cervix (>4 cm) Membrane prolapse beyond the external OS.
- 11. CERVICAL INSUFFICIENCY • Cervix starts dilating and effacing before her pregnancy has reached term, usually between 16–28 weeks of gestation, without any associated pain or uterine contractions. 1/9/2024
- 12. • Cervical incompetence is probably responsible for causing 20% to 25% of miscarriages in the second trimester. • The woman gives history of recurrent second trimester pregnancy losses, occurring earlier in gestation in successive pregnancies and usually present with a significant cervical dilatation of 2 cm or more in the early pregnancy. • However, usually there is absence of any other symptoms. In the second trimester, cervix may dilate up to 4 cm in association with active uterine contractions. • This may be associated with rupture of the membranes resulting in the spontaneous expulsion of the fetus. 1/9/2024
- 13. • On clinical examination, the cervical canal may be dilated and effaced. Fetal membranes may be visible through the cervical os. • Sonographic serial evaluation (every two weeks) of the cervix for funneling and shortening in response to transfundal pressure has been found to be useful in the evaluation of incompetent cervix. 1/9/2024
- 14. Other findings observed on ultrasound examination include the following: • Cervical length < 25mm. However finding of the short cervical length on TVS is not a confirmed diagnostic test for incompetent cervix. It could also be due to early preterm labor. • Protrusion of the membranes. • Presence of the fetal parts in the cervix or vagina. • Cervical dilation and effacement with the changes in form of T, Y, V, U (can be remembered using the mnemonic “Trust Your Vaginal Ultrasound”) • Another important finding on TVS examination of cervical incompetence is funneling. Funneling implies herniation of fetal membranes into the upper part of endocervical canal. However this too is not diagnostic of incompetent os. 1/9/2024
- 15. 1/9/2024
- 16. 1/9/2024
- 17. Non-Pregnant State • The Internal OS allows the passage of No. 8 Hegar’s Dilator or foley’s catheter filled with 1 ml water without resistance. • Premenstrual hysterocervicography will show the typical funneling of internal OS. 1/9/2024
- 18. PRESURGICAL PREPARATION • Contraindications to cerclage include bleeding, contractions, or ruptured membranes, any of which substantially raise the likelihood of labor and failure. • Prophylactic elective cerclage before dilation is preferable, timing between 12 and 14 weeks’ gestation allows early intervention. • Still, it avoids surgery in the first trimester, which is when most predestined spontaneous losses occur, and screening or aneuploidy and malformation is completed. • Cervical neoplasia screening in suitable candidates and gonorrhea and chlamydial infection testing are done. 1/9/2024
- 19. PRESURGICAL PREPARATION • Obvious cervical infection is treated. • At times, the cervix instead is found to be dilated, effaced, or both, and an emergency cerclage is performed • In more-advanced pregnancy, the risk of stimulating preterm labor or of rupturing membranes with the surgery is greater. 1/9/2024
- 20. • Regional analgesia is suitable and preferred then placed in standard lithotomy position. • The vagina and perineum are cleaned For surgery and the bladder is drained. • Some operators do not use potentially irritating antiseptic solution in amnionic membranes are exposed and instead use warm saline • For suturing, options include a no. 1 or 2 nylon or polypropylene monofilament suture or 5-mm Mersilene tape. • During placement, the suture is placed as cephalad along the cervical length as possible, is anchored into the dense cervical stroma, yet avoids the bladder. Two tandem cerclage suture rings are not more effective than one 1/9/2024
- 21. • Emergency cerclage placement with a thinned dilated cervix is more difficult, and tissue tearing and membrane puncture are risks. • Gentle replacement of the prolapsed amnionic sac back into the uterus can aid suturing. Options include steep terendelenburg or flling the bladder with 600 mL of saline through a Foley catheter in the bladder. However, these steps may carry the cervix cephalad and away from the operating field. • Instead, membranes can be pushed inward by a wide, moist sponge stick. • A Foley catheter can instead be inserted through the cervix, and infation of the 30-mL balloon can detect the amnionic sac inward. • The balloon is gradually defated as the cerclage suture is tightened around the catheter tubing, which is then removed. With any of these, simultaneous gentle outward traction created by ring forceps placed on the cervical edges may be helpful. 1/9/2024
- 22. STEPS OF SHIRODKAR’S OPERATION Step I: The patient is put under light general anesthesia and placed in lithotomy position with good exposure of the cervix by a posterior vaginal speculum. The lips of the cervix are pulled down by sponge holding forceps or Allis tissue forceps. Step II: A transverse incision is made anteriorly below the base of the bladder on the vaginal wall and the bladder is pushed up to expose the level of the internal os. A vertical incision is made posteriorly on the cervicovaginal junction. Step III: The nonabsorbable suture material—Mersilene (Dacron) or Ethibond tape is passed submucousl with the help of an aneurysm needle or cervical needle so as to bring the suture ends through the posterior incision. Step IV: The ends of the tapes are tied up posteriorly by a reef knot. The bulging membranes, if present, must be gently reduced beforehand into the uterine cavity. The anterior and posterior incisions are repaired by interrupted stitches using chromic catgut. 1/9/2024
- 23. 1/9/2024
- 24. Shirodkar technique: • A high transvaginal purse string suture placed following bladder mobilization to allow insertion above cardinal ligaments.
- 26. McDONALD’S OPERATION • The nonabsorbable suture (Mersilene) material is placed as a purse-string suture as high as possible (level of internal os) at the junction of the rugose vaginal epithelium and the smooth vaginal part of the cervix below the level of the bladder. • The suture starts at the anterior wall of the cervix. Taking successive deep bites (4–5 sites), it is carried around the lateral and posterior walls back to the anterior wall again where the two ends of the suture are tied.
- 28. 1/9/2024
- 29. • During procedure, risk of tissue tearing and membrane rupture is more. • To prevent this, steep Trendelenburg’s or filling the bladder with 600ml of normal saline through an Foley's catheter. • For uncomplicated pregnancy without labor , cerclage is usually cut and removed at 37 weeks of gestation.
- 30. • Wurm’s procedure: • Also known as Hefner’s cerclage, it is done by application of U or mattress sutures and is of benefit when minimal amount of length of cervical canal is left.
- 31. • Lash procedure • This surgical procedure is usually performed in nonpregnant woman. It is usually performed for an anatomical defect in cervix resulting from cervical trauma. • In this surgery, the cervical mucosa is opened anteriorly, bladder reflected and the cervical defect repaired with interrupted transverse sutures before closing the vaginal mucosa.
- 32. Contraindications for cerclage • Uterine contractions/bleeding. • Clinical evidence of Chorioamnionitis. • Premature rupture of membranes. • Cervical dilatation of more than 4 cm • Polyhydramnios • Fetal anomaly incompatible with life. ● Women with Mullerian anomalies. ● Previous cervical surgery. ● Multiple dilatation and evacuation. 1/9/2024
- 33. Risks of cerclage • Premature rupture of the membranes • Chorioamnionitis • Preterm labor • Cervical laceration or amputation resulting in the formation of scar tissue over the cervix • Bladder injury • Maternal hemorrhage • Cervical dystocia • Uterine rupture, vesicovaginal fistula 1/9/2024
- 34. Removal of cerclage • Transvaginal cerclage should be removed before labor, usually 36 and 37 weeks of gestation. • In women in establishing preterm labor, cerclage should be removed to minimize cervical trauma. • A Shirodkar suture usually require anesthesia to remove. • All women with transabdominal cerclage, require delivery by caesarean section.
- 35. REMOVAL FOLLOWING PPROM (24-34) WEEKS • Without evidence of infection or preterm labour, delayed removal of the cerclage for 48 hours can be considered, for a course of prophylactic steroids and/or in utero transfer. • Delayed suture removal until labour is a/w an increased risk of maternal/fetal sepsis and is not recommended. • Should be removed immediately following PPROM before 23 weeks and after 34 weeks.
- 36. Alternative to cervical cerclage • may be bed rest alone to avoid pressure on the cervix. • Injection of 17a-hydroxyprogesterone caproate 500 mg IM weekly is given as cervical incompetence is considered as a continuum of preterm birth syndrome. • Use of vaginal pessary, when cervix is found short on ultrasound, is found helpful.
- 37. Advice on discharge • (a) Usual antenatal advice. • (b) To avoid intercourse. • (c) To avoid rough journey. • (d) To report if there is vaginal bleeding or abdominal pain. • (e) Periodic ultrasonographic monitoring of the fetus and the cervix.
- 38. References
- 39. 1/9/2024
Editor's Notes
- There is no evidence to support to laparoscopic approach over laparotomy abdominal cerclage. Management of a delayed miscarriage or fetal death with an abdominal cerclage. Senior involvement Suction curettage or by dilatation and evacuation through the stick by up to 18 WOG Alternatively cut the suture usually via a posterior colpotomy Failing this a hysterectomy or cesarean section may be required
- Rescue cerclage, where the cervix is already open and the fetal membranes exposed.
- It can be ollowed by prolapse and ballooning o the amnionic membranes into the vagina, and ultimately, expulsion o an immature etus. Tis sequence oten repeats in uture pregnancies. women with prior cervical conization ound a ourold risk o pregnancy loss beore 24 weeks’ gestation. Te physical nding o early dilation o the internal cervical os and visible membranes is another indicator o insufciency.
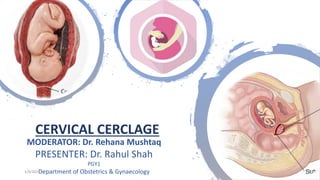
- Table 9.4: Risk factors for development of cervical incompetence Diagnosis of cervical incompetence in a previous pregnancy Previous history of preterm premature rupture of membranes History of diethylstilbestrol exposure, which can cause anatomical defects in uterus and cervix History of previously having received trauma to the cervix Fig. 9.3A: Anatomical changes in the endocervical canal associated with cervical incompetence Fig. 9.3B: Ultrasound changes in endocervical canal with cervical incompetence a normal cervix. As the internal cervical os opens and the membrane start herniating into the upper part of endocervical canal, the cervical shape on ultrasound changes into a Y. With the further progression of above mentioned cervical changes, Y shape changes into U. • Another important fi nding on TVS examination suggestive of cervical incompetence is funneling. Funneling implies herniation of fetal membranes into the upper part of endocervical canal. However this too is not diagnostic of incompetent os. Some of the tests for diagnosing cervical incompetence, which were previously used and are still used at some places, include the following: Passage of a No. 8 (8 mm) Hegar dilator, traction using an intrauterine Foley catheter, etc.
- T-shaped cervix on ultrasound examination points towards a normal cervix. As the internal cervical os opens and the membrane start herniating into the upper part of endocervical canal, the cervical shape on ultrasound changes into a Y. With the further progression of above mentioned cervical changes, Y shape changes into U.
- When either technique is perormed electively, women with a classic history o cervical insufciency have good outcomes (Caspi, 1990; Kuhn, 1977). For either vaginal or abdominal cerclage, evidence is insufcient to recommend perioperative antibiotic prophylaxis
- In ths video we will see shirodhkar technique U shape buldging and cervical os Merselline Infiltration with cold normal saline Dissection in oubovesical fascia upto ridge Start in anti clock wise Needle is drive through ant lip of cervix taking half the thickness of the cervix Once we reach 11 then we go to 9 then 7 o clock then posterior wall of the cervix then 6 o clock Then another neddle in clockwise 1 o clock 3 o clock then 6 o clock Then end of needle cut and both end are tied Surgeons knot then 3 more knot each knot has to be square Loop is kept in posterior cervix so that it cn be cut in 37 week or onset of labor Check the bleeding Then use chromic catgut continuous or interrupted Entire is sutured so the foreign body is not exosed so there is less secretion Avoid deep bite to prevent bladder injury This is more anatomical than mcd it prevents preterm delivery or seconnd trimester abortion as it is in level of internal os Less chace of chorioamniotis Tho external os becomes patoulous, internal od is closed Thank you very much for your patience listening
- McDonald cerclage procedure for incompetent cervix. A. Start of the cerclage procedure with a no. 2 monofilament suture being placed in the body of the cervix very near the level of the internal os. B. Continuation of suture placement in the body of the cervix so as to encircle the os. C. Encirclement completed. D. The suture is tightened around the cervical canal sufficiently to reduce the diameter of the canal to 5 to 10 mm, and then the suture is tied. The effect of the suture placement on the cervical canal is apparent. A second suture placed somewhat higher may be of value if the first is not in close proximity to the internal os.