Anatomy of The Heart.pptx
•Download as PPTX, PDF•
0 likes•373 views

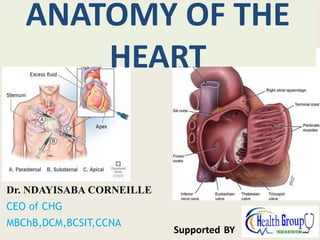
The pericardium is the sac that encloses the heart. It consists of an outer fibrous part known as the fibrous pericardium, and a double layered serous sac known as the serous pericardium. The pericardium prevents sudden dilatation of the heart, especially the right chamber, and displacement of the heart and great vessels, minimizes friction between the heart and surrounding structures, and prevents the spread of infection or cancer from the lung or pleura.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Anatomy of The Heart.pptx
Similar to Anatomy of The Heart.pptx (20)
More from Dr Ndayisaba Corneille
More from Dr Ndayisaba Corneille (20)
Recently uploaded
Recently uploaded (20)
Anatomy of The Heart.pptx
- 1. ANATOMY OF THE HEART Dr. NDAYISABA CORNEILLE CEO of CHG MBChB,DCM,BCSIT,CCNA Supported BY
- 2. THE PERICARDIUM • The pericardium is the sac that encloses the heart. It consists of an outer fibrous part known as the fibrous pericardium, and a double layered serous sac known as the serous pericardium. • The pericardium prevents – sudden dilatation of the heart, especially the right chamber, and displacement of the heart and great vessels, – minimizes friction between the heart and surrounding structures, and – prevents the spread of infection or cancer from the lung or pleura. Dr Ndayisaba Corneille
- 3. The fibrous pericardium • The fibrous pericardium servers to limit the sudden distention of the heart, it is conical in shape and has an apex and a base, anterior and a posterior surface. Dr Ndayisaba Corneille
- 4. The serous pericardium • The serous pericardium has both a parietal layer and a visceral layer. The parietal layer lines the inside of the fibrous pericardium while the visceral layer lines the heart and the vessels entering it. • This layer is also known as the epicardium of the heart. The serous pericardium gives rise to two sheaths – A venous serous sheath and arterial serous sheath. Dr Ndayisaba Corneille
- 5. CONTENTS OF THE PERICARDIUM • Pulmonary trunk • Ascending aorta • Terminal ends of inferior vena cava and • superior vena cava • Right and left pulmonary veins • The heart. Dr Ndayisaba Corneille
- 6. BLOOD SUPPLY, NERVE SUPPLY • Blood is supplied by branches from the internal thoracic artery, and musculophrenic artery and from the descending aorta. • Its venous drainage is from tributaries that empty into the azygous system of veins. • It is supplied by branches arising from the vagus, phrenic and sympathetic trunk. Dr Ndayisaba Corneille
- 7. APPLIED ANATOMY: Pericardial effusion • The potential space between the parietal and visceral layers of the s erous pericardium normally contain s a small volume of fluid. • Excess fluid is termed a pericardial effusion. If t he volume is sufficiently large, this can reduce ventricular filling as a consequence of the lack of elasticity of the fibrous pericardium and this is termed • cardiac tamponade. In severe cases , this can cause heart failure. Dr Ndayisaba Corneille
- 8. Cardiac Tamponade – Cardiac enlargement or chronic pericardial effusions, both of which develop slowly, will stretch the fibrous pericardium. – However, the fibrous pericardium cannot stretch acutely, and the rapid accumulation of as little as 200 mL of fluid can result to fatal cardiac tamponade. Dr Ndayisaba Corneille
- 9. Pericardiocentesis and Pericardial puncture • pericardiocentesis is the drainage of the excess fluid through insertion of a needle as may be required to alleviate tamponade. • Pericardial puncture is carried out close to the medial or sternal end of the right 5th to 6th costal cartilage near the margin of the sternum (Parasternal) to avoid puncture of the internal thoracic artery. It can also be made close to the xyphoid process i.e. left xiphicostal angle (Substernal); the syringe is passed upwards and backwards to enter the pericardium. • Hemopericardium results from perforation of either the heart or the intrapericardial great vessels Dr Ndayisaba Corneille
- 10. Epicardial deposit of fat • In obese subjects, excessive epicardial deposit of fat may encase the heart, but because pericardial fat is liquid at body temperature, cardiac motion is generally unhindered Dr Ndayisaba Corneille
- 11. THE HEART A human heart viewed from the so-called anterior position, demonstrating the valentine heart orientation. The red line surrounding the heart is the characteristic symbol, which was theoretically derived from observing the heart in this orientation .
- 12. Dr Ndayisaba Corneille External Heart: Anterior View Figure 18.4b
- 13. THE HEART • The heart is a pair of muscular pump with valves that is combined into a single organ. • Although it is composed of a fibromuscular skeleton and conducting tissues that are structurally interwoven, they are functionally i.e physiologically differentiated into right & left parts. Dr Ndayisaba Corneille
- 14. DEVELOPMENT OF THE HEART • The heart starts developing from the 3rd week of intrauterine life. • By the formation of two parallel cardiogenic cords. • The cords become canalized to form two endothelial tubes referred to as endocardial heart tubes. Dr Ndayisaba Corneille
- 15. • the two heart tubes will fuse together to form a tubular vessel with one chamber. Which is attached to the dorsal wall by a dorsal mesentery known as Mesocardia. Dr Ndayisaba Corneille
- 16. As the heart develops it later forms 5 saculations known as:- Truncus Arteriosus, Bulbos Cordis, Primitive ventricle, Primitive Atrium, and Sinus Venosus Dr Ndayisaba Corneille
- 17. • As the heart increases in length its mesocardia does not allow it to grow upwards out of the future pericardial sac and so developing heart begins to form an S - shaped tube. • Its two caudal segments the sinus venosus and primitive Atrium comes to lie dorsal to the three cephalic segments. Dr Ndayisaba Corneille
- 18. • The truncus arteriosus divides to form the ascending aorta and the pulmonary trunk. • A definite ventricle is formed from the bulbus cordis and primitive ventricle, Dr Ndayisaba Corneille
- 19. • while the definite Right Atrium are formed from the right half of the primitive atrium and the right half of the sinus venosus. • Actually the left half of the sinus venosus disintegrates. • Therefore the left atrium is formed from the left half of the primitive atrium and the developing pulmonary veins. Dr Ndayisaba Corneille
- 20. • The 2 atria lies posterior while the two ventricles lie anterior but later the heart will undergo a slight rotation to the left and on its long axis and so the following events occurs. Dr Ndayisaba Corneille
- 21. • The right atrium is now largely anterior partly posterior forming the right border • The left atrium comes to lie posterior • The right ventricle comes to lie largely in front and slightly inferior. • The left ventricle comes to lie largely inferior and slightly in front forming the apex of the heart and the left border. • The interatrial and interventricular septa comes to face forward. Dr Ndayisaba Corneille
- 22. THE ADULT HEART • The heart is conical in shape, and possess an apex and four surfaces. Which include – the base (posterior surface) – a sternocostal (anterior surface) – a left Surface – and a diaphragmatic surface (inferior surface). Dr Ndayisaba Corneille
- 23. • Location • The Heart is situated in the mediastinum of the thoracic cavity, enclosed in the pericardium. • It is somewhat pyramidal in shape and placed obliquely behind the sternum so that 1/3rd of the heart is to the right of median plane and 2/3rd of the heart is to the left of the median plane. Dr Ndayisaba Corneille
- 24. In infants the heart is about 1/130 of the body weight while in adult it is about 1/300 of body weight. Therefore the heart is relatively larger in infants than in adults. Dr Ndayisaba Corneille
- 25. The Base • The Base is directed upwards and backwards. • It is situated posteriorly opposite the T5 to T8 vertebra. • It is formed mainly by the left atrium • Between it and the thoracic vertebra lies the pericardium, oesophagus, descending aorta, vagus nerve and thoracic duct. Dr Ndayisaba Corneille
- 26. The apex • The apex of the heart is rounded. • It is formed by the left ventricle and is at the level of the fifth left intercostal space, 9cm from the midline. At this position the apex beat is heard. • The apex of the heart is pointing inferiorly and to the left, causing the long axis of the heart to be at an acute angle to the long axis of the body Dr Ndayisaba Corneille
- 27. The sternocostal surface • The Sternocostal surface is formed mainly by the right ventricle, part of the right atrium and right Auricle and a small part of the left ventricle. • The Sternocostal surface presents two grooves an anterior Interventricular sulcus and the atrioventricular sulcus. Dr Ndayisaba Corneille
- 28. The left surface • The left surface is formed by the left ventricle. At the upper end is part of the left atrium and the left auricle. Dr Ndayisaba Corneille
- 29. The diaphragmatic surface • The diaphragmatic surface resting on the central tendon of the diaphragm is formed by the right and left ventricles which is demarcated by the posterior interventricular sulcus. Dr Ndayisaba Corneille
- 30. The heart is composed of four chambers. The right and left atria The right and left ventricles. CHAMBERS OF THE HEART Dr Ndayisaba Corneille
- 31. DEMARCATION OF CHAMBERS OF THE HEART ON THE SURFACE • On the surface the chambers of the heart are demarcated or delineated by the following 3 grooves: • A. Coronary sulcus (atrioventricular groove). • B. Anterior interventricular sulcus. • C. Posterior interventricular sulcus Dr Ndayisaba Corneille
- 32. The right atrium: EXTERNAL FEATURES • A. The right atrium is elongated vertically with the superior vena cava (SVC) at its upper end and the inferior vena cava(IVC) at its lower end. • • B. The upper anterior part presents the right auricular appendage, the right auricle. • C. A shallow vertical groove referred to as sulcus terminalis extends along the right border between the superior and inferior vena cavae Dr Ndayisaba Corneille
- 33. INTERIOR OF THE RIGHT ATRIUM • On opening the atrium, a ridge – the crista terminalis is seen to correspond in position to the sulcus terminalis on the exterior indicates were the two primitive chambers merge. • The portion of the atrium behind the crista is smooth, this part develops from the sinus venosus. • The portion in front is trabeculated: it develops from the primitive atrium. Dr Ndayisaba Corneille
- 34. • The parallel ridge running forward from the crista terminales towards the auricle are called musculipectinati (peten a comb). • From the lower end of the crista terminales a prominent fold of endocardium which represents fetal valve of the IVC, (though imperfect) passes in front of the orifice of the IVC Dr Ndayisaba Corneille
- 35. • This imperfect small valve become continues with the crescentic margin of a depression the fossa ovalis • which is situated in the interatrial septum which forms the medial wall of the right atrium. Dr Ndayisaba Corneille
- 36. • The right atrioventricular orifice replaces the anterior wall. • The orifice of the coronary sinus opens between the orifice of the IVC and the tricuspid orifice. • It is also guarded by a fold which arises from the valve of IVC. Dr Ndayisaba Corneille
- 37. • There is also the intervanous tubercle of Lower which is a very small projection at the posterior wall of the atrium just below the orifice of SVC. • During IUL it directs SVC blood to the right ventricle. Dr Ndayisaba Corneille
- 38. LEFT ATRIUM • The left atrium forms 2/3rd of the posterior surface of the heart, though its auricle extends up to the left border. • It is demarcated from the left ventricle below by the coronary sulcus. • The right and left pulmonary veins open into it, near the right and left margins. Dr Ndayisaba Corneille
- 39. The interior of the left atrium • In the interior of the left atrium the auricle is trabeculated, the rest part is smooth, • the mouths of the four pulmonary veins open on the posterior wall. • The left atrioventricular orifice and the interatria septum replaces the anterior wall. Dr Ndayisaba Corneille
- 40. • The septal wall shows the fossa lunata which corresponds to the fossa ovalis of the right atrium. • the rough part of the atrium is derived from the primitive atrium while the smooth part is formed as a result of absorption of the developing pulmonary veins. • Nothing is obtained from the left horn of the sinus venosus. Dr Ndayisaba Corneille
- 41. VENTRICLES • The ventricles – right and left lie in front of their atria. • They form the apex of the heart, the entire inferior margin and diaphragmatic surface, most of the left margin and sternocostal surface, and a very small part of the base. Dr Ndayisaba Corneille
- 42. VENTRICLES • On cross section it is seen that the thickness of the two ventricles is proportion to the amount of work each has to do. • The left ventricle is the pump of the systemic system while the right ventricle is the pump to the pulmonary system, so the ratio of their thickness is 3:1. Myocardium of left ventricle is much thicker than the right. Dr Ndayisaba Corneille
- 43. THE RIGHT VENTRICLE: • This is the chamber of the heart which receives blood from the right atrium and pumps it out through the pulmonary trunk to the lungs where the blood is oxygenated. • It is triangular in shape but in cross section it is crescentic in shape due to the bulging of the interventricular septum into its cavity. Dr Ndayisaba Corneille
- 44. • It is separated from the right atrium by the coronary sulcus. Dr Ndayisaba Corneille
- 45. The interior of the right ventricle • The interior of the right ventricle presents muscular bundles called trabeculae carneae which correspond to the part derived from the primitive ventricle. • Some of muscle bundles are merely elevated ridges, • other are attached at both ends like bridge, this is the septomarginal band or moderator band through which passes the right fasciculus of atrioventricular bundle of HIS Dr Ndayisaba Corneille
- 46. • others form finger like projections called the papillary muscles which here are present anterior, posterior and septal papillary muscles. • From the apex of these papillary muscles arises the chordae tendinae which attaches it to the ventricular surface of the atrio ventricular valves. Dr Ndayisaba Corneille
- 47. • The smooth out flowing part of the right ventricle is referred to as the infundibulum. • It is the conical upper 2.5cm of the right ventricle that give rise to the pulmonary trunk. It is derived from the bulbous cordis. • The two parts are separated by a muscular ridge called the supra ventricular crest, which lies between the tricuspid valve and pulmonary orifice. Dr Ndayisaba Corneille
- 48. THE LEFT VENTRICLE • The left ventricle is the heart chamber that pumps oxygenated blood which enters it through the left atrium to the systemic circulatory system through the aorta. • The left ventricle forms part of the sternocostal, diaphragmatic and left border of the heart. • It also forms the apex of the heart which lies at the 5th intercostal space where the apex beat is felt. Dr Ndayisaba Corneille
- 49. • The cavity of the left ventricle is longer then that of the right ventricle. It is also circular in cross section. • It has two parts – a rough area that presents the trabeculae carneae. It develops from the primitive ventricle. Dr Ndayisaba Corneille
- 50. THE INTERVENTRICULAR SEPTUM • The interventricular septum is fleshy, except at its uppermost part which is membranous. • The fleshy or muscular part is an out growth from the apex of the heart, • the membranous part is an out growth from the interatrial septum and right side of the root of the aorta. Dr Ndayisaba Corneille
- 51. • Failure of the fleshy and membranous parts to fuse results in an interventricular septal defect with subsequent leakage into the right ventricle from the high pressured left ventricle. Dr Ndayisaba Corneille
- 52. The valves of the heart • The valves of the heart is destined to ensure that there is one-way directional flow of the circulating blood. • The valves of the heart include: – The right and left atrio ventricular valves – Pulmonary and aorta semiluna valves. Dr Ndayisaba Corneille
- 53. The right atrioventricular valves is tricuspid and the left is bicuspid. Both valves have fibrous rings to which the cusps are attached. Dr Ndayisaba Corneille
- 58. Venous drainage…. Venous blood from heart drains into right atrium through a.Coronary sinus b.Anterior cardiac veins c. Venae cordis minimae (thebesian veins) Dr Ndayisaba Corneille
- 59. • 2 to 3cm long • Situated – left posterior coronary sulcus • Opens – right atrium. • Valve- Thebasian valve Tributaries are….. 1.Great cardiac vein begins apex, and ascends through the anterior Interventricular groove, traverses – coronary sulcus. It receives left marginal vein. 2.Small cardiac vein passes along right posterior coronary sulcus. A.Coronary sinus….. Dr Ndayisaba Corneille
- 60. 3.Middle cardiac vein Begins – apex, traverses – PIG, ends – middle of coronary sinus. 4.Posterior vein of left ventricle Present on diaphragmatic surface of left ventricle. 5.Obligue vein of left atrium(vein of Marshall) Descends obliquely – back of left atrium Dr Ndayisaba Corneille
- 61. Drains anterior part of right ventricle…. Usually 2 or 3 in number- parallel to each other. Opens to right atrium. B.Anterior cardiac veins… Dr Ndayisaba Corneille
- 62. • Opens into all chambers. • Numerous in right atrium & ventricle. .Venae cordis minimae/Thebesian veins… Dr Ndayisaba Corneille
- 64. Applied anatomy • An atrial septal defect is a birth defect of the heart in which there is a hole in interatrial septum of the heart. • The hole can vary in size and may close on its own or may require surgery Dr Ndayisaba Corneille
- 65. Ventricular Septal Defect • A ventricular septal defect (VSD) is a birth defect of the heart in which there is a hole in the interventricular septum of the heart Dr Ndayisaba Corneille
- 66. END Dr Ndayisaba Corneille THANKS FOR LISTENING By DR NDAYISABA CORNEILLE MBChB,DCM,BCSIT,CCNA Contact us: amentalhealths@gmail.com/ ndayicoll@gmail.com whatsaps :+256772497591 /+250788958241