7. The
Conscience
of EMS
JOURNAL OF EMERGENCY MEDICAL SERVICES
38
I Beyond the Tape I
Law enforcement officers make major impact
as initial care providers
B
y David Kleinman, NREMT-P, Tammy Kastre, MD
May 2012 Vol. 37 No. 5
Contents
I 62
46 I Prepared for the Worst I
Tactical training offers many benefits to EMS
By William Justice, NREMT-P; Lt. Kerry Massie, NREMT-I; Jeffrey M. Goodloe,
MD, NREMT-P, FACEP
52 I Partners in Crime I
EMS provides a training program for local law enforcement
By Capt. Mario Ramirez, MD, MPP; Andrew N. Pfeffer, MD; Greg Lee; Corey M.
Slovis, MD, FACEP
56 I hat’s buggin’ ems I
W
Departments columns
9 I Load go I Now on JEMS.com
14 I EMS in Action I Scene of the Month
16 I From the Editor I On the Front Lines
By A.J. Heightman, MPA, EMT-P
18 I Letters I In Your Words
20 I Priority Traffic I News You Can Use
24 I LEADERSHIP SECTOR I Crisis Management
B
y Gary Ludwig, MS, EMT-P
27 I Management Focus I Extra Set of Hands
y Richard Huff, NREMT-B
B
30 I Tricks OF the TRADE I Numbers
B
y Thom Dick
32 I case of the month I Miracle in the Desert
B
y Jeff Westin, MD; Pat Songer, NREMT-P, ASM; Kelly Buchanan,
MD; Loren Gorosh, MD; Ryan Hodnick, DO; Bryan E. Bledsoe,
DO, FACEP, FAAEM
36 I Research review I What Current Studies Mean to EMS
B
y David Page, MS, NREMT-P
How to rid your rigs of a bedbug infestation
By Wayne M. Zygowicz, BA, EFO, EMT-P
62 I Breaking Barriers I
Practice cultural sensitivity to provide care to immigrant
communities
By Keith Widmeier, NREMT-P, CCEMT-P, EMS-I, BA; Emily Coffey, BA,
NREMT-P
68 I ultiple Airways I
M
Rapid assessment is key for managing numerous patients
By Paul E. Phrampus, MD
I 68
74 I Ad Index
75 I employment Classified Ads
78 I The Lighter Side I Zombie EMS
B
y Steve Berry
82 I LAST WORD I The Ups Downs of EMS
About(Ariz.) Sheriff’s Department deputy demonstrates the value of early law enforcement officer delivery of EMS treatment, particularly at an active-shooter incident or
the Cover
A Pima County
situations where it’s unsafe for EMS to enter. Find out how training and equipping first-arriving police officers, sheriff’s deputies and highway patrol officers can help save patients (and other
officers) in “On the Front Lines,” p 16; “Beyond the Tape,” pp 38–45; “Prepared for the Worst,” pp. 46–51; and “Partners in Crime,” pp. 52–55. Photo Matthew Strauss
Premier Media Partner of the IAFC, the IAFC EMS Section Fire-Rescue Med
www.jems.com
MaY 2012
JEMS
7
9. LOAD GO
log in for EXCLUSIVE CONTENT
A Better Way to Learn
JEMSCE.com
online continuing
education program
n
Photo Gary Jackson
Innovators Dine
The EMS 10: Innovators in EMS award winners pose at the dinner where they were honored for their achievements. Pictured from top left are Tom Bouthillet, Michael Millin, Seth Hawkins, Will Smith, Pat Songer,
Rob Lawrence, Stephanie Haley-Andrews and David Reinis. Not pictured are Mary Meyers, Paul Paris,
E. Reed Smith and Todd Stout. In case you’ve missed the past winners of this annual award, make sure
to check them out at jems.com/ems10
us o
follow
JEMS.com offers you
original content, jobs,
products and resources.
But we’re much more
than that; we keep
you in touch with
your colleagues
through our:
Facebook fan page;
JEMS Connect site;
Twitter account;
LinkedIn profile;
Product Connect site; and
Fire EMS Blogs site.
like us
facebook.com
/jemsfans
Sponsored Product Focus
Speechmike
With more than 50 years of experience in the voice technology market, Philips Speech
Processing provides innovative, practical dictation and transcription solutions that allow
professionals to increase productivity and efficiency. As the leading dictation device on
the market, the SpeechMike is specifically designed to enhance productivity for optimal
speech recognition results. Its ergonomic, intuitive design boasts dictation control, playback speakers, and PC navigation in a single device, and it allows users to send sound
files for transcription at the press of a button.
s Check out their ad on JEMS.com!
May poll question
follow us
twitter.com
/jemsconnect
get connected
linkedin.com/groups?
about=gid=113182
How do you celebrate EMS Week?
April Poll Results
Which is a more dangerous location for
EMS providers driving an ambulance?
34%
27%
39%
I
nterstate or rural highway
Rural streets
p y agency hosts an event.
M
p recognize it with coworkers.
I
p don’t even know when it is!
I
p
Other
ems news alerts
To vote, do a keyword search on JEMS.com for “polls.”
s jems.com/poll2012/
Check it out
jems.com/enews
jems.com/ems-products
Suburban streets.
The mobile version
s http://m.jems.com/poll/
best bloggers
FireEMSBlogs.com
www.jems.com
MAY 2012 JEMS
9
10. Conscience
of EMS
JOURNAL OF EMERGENCY MEDICAL SERVICES
The
Conscience
of EMS
JOURNAL OF EMERGENCY MEDICAL SERVICES
Editor-In-Chief I A.J. Heightman, MPA, EMT-P I a.j.heightman@elsevier.com
MANAGING Editor I Jennifer Berry I je.berry@elsevier.com
associate eDITOR I Lauren Hardcastle I l.hardcastle@elsevier.com
assistant eDITOR I Allison Moen I a.moen@elsevier.com
assistant eDITOR I Kindra Sclar I k.sclar@elsevier.com
online news/blog manager I Bill Carey I bill@goforwardmedia.com
Medical Editor I Edward T. Dickinson, MD, NREMT-P, FACEP
Technical Editors
Travis Kusman, MPH, NREMT-P; Fred W. Wurster III, NREMT-P, AAS
Contributing Editors I Bryan Bledsoe, DO, FACEP, FAAEM; Ann-Marie Lindstrom
Editorial Department I 800/266-5367 I editor.jems@elsevier.com
art director I Liliana Estep I alildesign@me.com
Contributing illustrators
Steve Berry, NREMT-P; Paul Combs, NREMT-B
Contributing Photographers
Mark C. Ide, Craig Jackson, Ray Kemp, Kevin Link, Julie Macie,
Jeffrey Mayes, Courtney McCain, Rick McClure, Tom Page, Rick Roach,
Steve Silverman, Chris Swabb, Grant Therrien, Raul Torres
Director of eProducts/Production I Tim Francis I t.francis@elsevier.com
Production Coordinator I Matt Leatherman I m.leatherman@elsevier.com
advertising director I Judi Leidiger I 619/795-9040 I j.leidiger@jems.com
Western Account Representative I Cindi Richardson I 661-297-4027 I
c.richardson@jems.com
senior Sales coordinator I Elizabeth Zook I e.zook@elsevier.com
Sales Administrative Coordinator I Liz Coyle I l.coyle@elsevier.com
SENIOR eMedia campaign manager I Lisa Bell I l.bell@elsevier.com
advertising department I 800/266-5367 I Fax 619/699-6722
marketing director I Debbie Murray I d.l.murray@elsevier.com
Marketing manager I Melanie Dowd I m.dowd@elsevier.com
Director, Audience Development Sales Support I Mike Shear I m.shear@elsevier.com
Audience development coordinator I Marisa Collier I m.collier@elsevier.com
SUBSCRIPTION DEPARTMENT I 888/456-5367
REprints, eprints Licensing I Wright’s Media I 877/652-5295 I reprints@jems.com
eMedia Strategy I 410/872-9303 I
Managing Director I Dave J. Iannone I dave@goforwardmedia.com
Director of eMedia Sales I Paul Andrews I paul@goforwardmedia.com
Director of eMedia Content I Chris Hebert I chris@goforwardmedia.com
EMS Today Conference Exposition
reed exhibitions I Christine Ford I 203/840-5391 I cford@reedexpo.com
ems today exhibit sales I 203/840-5611
Jeff Stasko I jstasko@reedexpo.com
elsevier public safety
vice president/publisher I Jeff Berend I j.berend@elsevier.com
founding editor I Keith Griffiths
founding publisher
James O. Page
(1936–2004)
Choose 16 at www.jems.com/rs
12. JOURNAL OF EMERGENCY MEDICAL SERVICES
The
Conscience
of EMS
JOURNAL OF EMERGENCY MEDICAL SERVICES
EDITORIAL board
William K. Atkinson II, PHD, MPH, MPA, EMT-P
President Chief Executive Officer
WakeMed Health Hospitals
James J. Augustine, MD
Medical Advisor, Washington Township (OH) Fire Department
Director of Clinical Operations, EMP Management
Clinical Associate Professor, Department of
Emergency Medicine, Wright State University
steve berry, NRemt-p
Paramedic EMS Cartoonist, Woodland Park, Colo.
Bryan E. Bledsoe, DO, FACEP, FAAEM
Professor of Emergency Medicine, Director, EMS Fellowship
University of Nevada School of Medicine
Medical Director, MedicWest Ambulance
Criss Brainard, EMT-P
Deputy Chief of Operations, San Diego Fire-Rescue
Chad Brocato, DHS, REMT-P
Assistant Chief of Operations, Deerfield Beach Fire-Rescue
Adjunct Professor of Anatomy Physiology, Kaplan University
J. Robert (Rob) Brown Jr., EFO
Fire Chief, Stafford County, Va., Fire and Rescue Department
Executive Board, EMS Section,
International Association of Fire Chiefs
carol a. cunningham, md, FACEP, FAAEM
State Medical Director
Ohio Department of Public Safety, Division of EMS
Thom Dick, EMT-P
Quality Care Coordinator
Platte Valley Ambulance
Marc Eckstein, MD, MPH, FACEP
Director of Prehospital Care, Los Angeles County/
USC Medical Center
Medical Director, Los Angeles Fire Department
Professor, Emergency Medicine,
University of Southern California
Charlie Eisele, BS, NREMT-P
Flight Paramedic, State Trooper, EMS Instructor
Bruce Evans, MPA, EMT-P
Deputy Chief, Upper Pine River Bayfield Fire Protection,
Colorado District
Jay Fitch, PhD
President Founding Partner, Fitch Associates
Ray Fowler, MD, FACEP
Associate Professor, University of Texas Southwestern SOM
Chief of EMS, University of Texas Southwestern Medical Center
Chief of Medical Operations,
Dallas Metropolitan Area BioTel (EMS) System
Adam D. Fox, DPM, DO
Assistant Professor of Surgery,
Division of Trauma Surgery Critical Care,
University of Medicine Dentistry of New Jersey
Former Advanced EMT-3 (AEMT-3)
Gregory R. Frailey, DO, FACOEP, EMT-P
Medical Director, Prehospital Services, Susquehanna Health
Tactical Physician, Williamsport Bureau of
Police Special Response Team
12
JEMS
MAY 2012
Jeffrey M. Goodloe, MD, FACEP, NREMT-P
Associate Professor EMS Division Director,
Emergency Medicine, University of Oklahoma School of
Community Medicine
Medical Director, EMS System for Metropolitan
Oklahoma City Tulsa
David E. Persse, MD, FACEP
Physician Director, City of Houston Emergency Medical Services
Public Health Authority, City of Houston Department. of Health
Human Services
Associate Professor, Emergency Medicine, University of Texas
Health Science Center—Houston
Keith Griffiths
President, RedFlash Group
Founding Editor, JEMS
John J. Peruggia Jr., BSHuS, EFO, EMT-P
Assistant Chief, Logistics, FDNY Operations
Dave Keseg, MD, FACEP
Medical Director, Columbus Fire Department
Clinical Instructor, Ohio State University
W. Ann Maggiore, JD, NREMT-P
Associate Attorney, Butt, Thornton Baehr PC
Clinical Instructor, University of New Mexico,
School of Medicine
Connie J. Mattera, MS, RN, EMT-P
EMS Administrative Director EMS System Coordinator,
Northwest (Illinois) Community Hospital
Robert J. McCaughan
Chief, City of Pittsburgh EMS
Chair, IAEMSC Metro Chief’s Section
Robin B. Mcfee, DO, MPH, FACPM, FAACT
Medical Director, Threat Science
Toxicologist Professional Education Coordinator,
Long Island Regional Poison Information Center
Mark Meredith, MD
Assistant Professor, Emergency Medicine and Pediatrics,
Vanderbilt Medical Center
Assistant EMS Medical Director for Pediatric Care,
Nashville Fire Department
Geoffrey T. Miller, EMT-P
Director of Simulation Eastern Virginia Medical School,
Office of Professional Development
Brent Myers, MD, MPH, FACEP
Medical Director, Wake County EMS System
Emergency Physician, Wake Emergency Physicians PA
Medical Director, WakeMed Health Hospitals Emergency
Services Institute
Mary M. Newman
President, Sudden Cardiac Arrest Foundation
Joseph P. Ornato, MD, FACP, FACC, FACEP
Professor Chairman, Department of Emergency Medicine,
Virginia Commonwealth University Medical Center
Operational Medical Director, Richmond Ambulance Authority
Jerry Overton, MPA
Chair, International Academies of Emergency Dispatch
David Page, MS, NREMT-P
Paramedic Instructor, Inver Hills (Minn.) Community College
Paramedic, Allina Medical Transportation
Member of the Board of Advisors,
Prehospital Care Research Forum
Paul E. Pepe, MD, MPH, MACP, FACEP, FCCM
Professor, Surgery, University of Texas
Southwestern Medical Center
Head, Emergency Services, Parkland Health Hospital System
Head, EMS Medical Direction Team,
Dallas Area Biotel (EMS) System
Edward M. Racht, MD
Chief Medical Officer, American Medical Response
Jeffrey P. Salomone, MD, FACS, NREMT-P
Associate Professor of Surgery,
Emory University School of Medicine
Deputy Chief of Surgery, Grady Memorial Hospital
Assistant Medical Director, Grady EMS
Kathleen S. Schrank, MD
Professor of Medicine and Chief,
Division of Emergency Medicine,
University of Miami School of Medicine
Medical Director, City of Miami Fire Rescue
Medical Director, Village of Key Biscayne Fire Rescue
John Sinclair, EMT-P
International Director, IAFC EMS Section
Fire Chief Emergency Manager, Kittitas Valley Fire Rescue
Corey M. Slovis, MD, FACP, FACEP, FAAEM
Professor Chair, Emergency Medicine,
Vanderbilt University Medical Center
Professor, Medicine, Vanderbilt University Medical Center
Medical Director, Metro Nashville Fire Department
Medical Director, Nashville International Airport
Barry Smith, EMT-P
CQI Coordinator, Regional EMS Authority (REMSA), Reno, Nev.
Walt A. Stoy, PhD, EMT-P, CCEMTP
Professor Director, Emergency Medicine,
University of Pittsburgh
Director, Office of Education,
Center for Emergency Medicine
Richard Vance, EMT-P
Captain, Carlsbad Fire Department
Jonathan D. Washko, BS-EMSA, NREMT-P, AEMD
Assistant Vice President, North Shore-LIJ Center for EMS
Co-Chairman, Professional Standards Committee,
American Ambulance Association
Ad-Hoc Finance Committee Member, NEMSAC
keith wesley, MD, facep
Medical Director, HealthEast Medical Transportation
Katherine H. West, BSN, MED, CIC
Infection Control Consultant,
Infection Control/Emerging Concepts Inc.
Stephen R. Wirth, Esq.
Attorney, Page, Wolfberg Wirth LLC.
Legal Commissioner Chair, Panel of Commissioners,
Commission on Accreditation of Ambulance Services (CAAS)
Douglas M. Wolfberg, Esq.
Attorney, Page, Wolfberg Wirth LLC
Wayne M. Zygowicz, BA, EFO, EMT-P
EMS Division Chief, Littleton Fire Rescue
14. EMS IN ACTION
Scene of the month
Photos Associated Press
High-PRofile Care
P
roviders from Southwest Ambulance prepare to initiate
the transfer of U.S. Rep. Gabrielle Giffords (D-Ariz.) to
TIRR Memorial Hermann Rehabilitation Hospital in Houston on
Jan. 26, 2011. Providers use extreme caution to provide followup treatment for Giffords’ critical head injury after she was
shot at a Congress On Your Corner event at a Safeway shopping
center outside of Tucson, Ariz. This high-profile case serves as
a reminder to EMS providers that they’re never able to predict
what patients they may have the opportunity to treat or transfer. Thanks to the excellent care delivered to Giffords and the
team effort between law enforcement and EMS, Giffords was
transported in a safe and coordinated manner and has made
outstanding progress in her recovery.
14
JEMS
MAY 2012
16. from the editor
putting issUes into perspective
by A.J. HEIGHTMAN, MPA, EMT-P
On the Front Lines
Updating the training care capabilities of law officers
Go to www.youtube.com/
watch?v=lBGfKtuo2AM
The clip shows a firefight that occurred on
the streets of Miami on April 11, 1986, between
eight FBI agents and two known murderers/
bank robbers: Michael Platt and William Matix.
Before the fight was over, multiple FBI agents
were killed by .223 gunshots from a Ruger
mini-14 in the hands of Michael Platt.
The brave FBI agents who were engaged in
this street battle were not armed with weapons
or ammunition that could make the most pronounced impact on their targets. Platt himself
had sustained 12 gunshot wounds (9 mm, .38
and 00 shot) but continued to fight.
This firefight and the resulting aftermath
resulted in dramatic changes in the way we
equip law enforcement officers. It was the genesis of the 10 mm and .40 SW rounds and use
of more advanced weaponry by law officers.
When I watched this powerful docudrama
in 1988, it dramatically affected me as an educator and EMS system planner. It also significantly changed the way I thought about
the EMS/law enforcement interface and the
need for better frontline care by (and for) police
officers and other members of the emergency
response family.
At this year’s National Association of
EMS Physician Conference in Tucson,
Ariz., in January, I heard a hidden message
during a keynote lecture by Brad Bradley,
EMT-P, of the Northwest Fire Rescue District,
and Joshua B. Gaither, MD, of the University
of Arizona Medical Center, on the mass shoot-
16 JEMS
MAY 2012
ing near Tucson involving Congresswoman
Gabrielle Giffords (D-Ariz.)
Gaither pointed out that the Pima County
Sheriff’s Department deputies who were in the
initial hot zone arresting the would-be assassin
and ensuring scene safety, used the recently
updated EMS training and small specialized law
enforcement Individual First Aid Kits (IFAKs) to
treat 14 of the 19 surviving victims.
In the early stages of this incident, the deputies retrieved their IFAKs, carried conveniently
behind the front headrest of their police cruisers, and used tourniquets and hemostatic clotting agents to control significant bleeding and
prevent the onset of shock. They also used
chest seals to seal open wounds and combat
tension pneumothorax.
It was a subtle statement that begged for
more explanation. So I contacted David
Kleinman, a detective with the Arizona
Department of Public Safety and a tactical
Photo Matthew Strauss
T
o truly understand the importance of
the content in the May 2012 issue of
JEMS, which focuses on updating the
training and equipment carried by law enforcement officers in your EMS system, I’d like you
to watch a gut-wrenching clip from the 1988
movie, In the Line of Duty. The clip is only eight
minutes long, but I think those eight minutes
will be some of the most stressful, and emotionally-charged of your career.
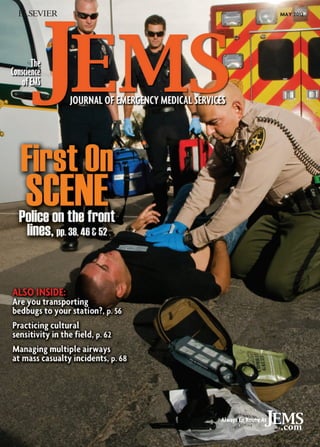
Contents of the Pima County Sheriff’s Dept IFAK.
paramedic with Pima Regional SWAT. I
learned that Kleinman had developed a specialized training program, called The First
Five Minutes, which was adopted by the Pima
County Sheriff’s Department.
That training, plus the up-to-date medical
supplies they carried in each patrol vehicle,
allowed the Pima County deputies to have a
major effect on the survival of many of the
victims at the Safeway shooting scene. The
content involved the most up-to-date treatment and supplies for hemorrhage control and
shock abatement.
Military research on the care rendered to critically injured soldiers in Iraq and Afghanistan
has shown that if you combat and control
hemorrhage before the onset of shock, mortality
decreases significantly.1 So this training for law
enforcement officers was not just up-to-date,
but it was also timely.
I asked David to write an article for this
month’s JEMS that detailed the training and
how it was used effectively to keep many of
the critically injured victims alive on Jan. 8,
2011. We found that several other innovative
law enforcement initiatives were implemented
in 2011 to train and equip officers to save
themselves when injured, save their colleagues
and save citizens during natural or man-made
disasters and mass casualty incidents. It was
clear to us that this new wave of updated training was significant and worthy of our attention, and yours.
The strong message for fire and EMS agencies is that law officers are often on the front
lines long before fire and EMS units arrive.
Please follow this educational trend, work to
have updated training provided to the law officers in your service area, and “arm” each officer
with the essential equipment they need to save
their lives and others.
The contents I believe each patrol officer
should carry in a compact gear pouch include:
4 compression dressing;
Hemostatic clotting agent dressing;
Tactical tourniquet;
Chest seal;
3 x 3 x 2 (gauze sponges);
4-1/2 Kerlix sterile roll bandages;
1 Transpore surgical tape;
Trauma shears;
Ventilation mask;
Three pair of Nitrile gloves; and
SAM Splint
The cost per kit is less than $100—but it’s a
small investment to save an officer or civilian
when time is critical. JEMS
References
1. Kragh J, Littrell M, Jones J, et al. Battle casualty survival
with emergency tourniquet use to stop limb bleeding.
J Emerg Med. 2011;41(6):590–597.
18. Photo Istockphoto.com
LETTERS
in your words
This month, Facebook users
chime in on “EMS Providers
Should Train like Fighters,” a
JEMS.com article by fitness columnist John Amtmann, EdD, on
why it’s important for EMS providers to train for the worst-case
scenario. Would you be prepared
to defend yourself? Also, users
share feedback on a March JEMS
article by Bryan Bledsoe, DO,
FACEP, FAAEM, on EMS in the Pennsylvania Amish community (“Simple Way
of Life: EMS in Amish country”).
Self Defense
I definitely think we should be prepared for any harmful
situation. I was involved in a situation that went bad
fast. I was assaulted by a patient who was on numerous
illegal drugs. Initially, he presented with hypoglycemic
symptoms, but after loading him into the unit, he began
to exhibit signs of paranoia and hallucinations. Luckily,
the police department was on scene, but unfortunately
he had a chance to grab me.
It took the fast thinking of the officer to physically
make him release his hold on me, and for my partner to
administer Versed, which did absolutely nothing, to get
me freed. It happened so fast, so I agree that it would
have been helpful if I’d known some self defense. That
way, I would have known how to break the death grip he
had on me when he wrapped his legs around me, without injuring him. He not only physically harmed me, but
he also made me lose the trust I had prior to that day.
Misty Bortz
Via Facebook
my own training to ensure scene safety by doing what
the rest on scene couldn’t.
I wrapped the patient up in a Brazilian Ju Jitsu hold.
Once I had him fully restrained, the officers assisted in
putting restraints on the man while they systematically
strapped both me and the patient to the backboard.
After we were both strapped in and he was much better
restrained, they loosened one strap at a time, so I could
slip my limbs out and prepare the patient for transport.
If a patient’s aggression causes this kind of situation,
knowing how to defend yourself is literally a lifesaver.
Joe Lee
Via Facebook
with people from all over the country and from all
walks of life.
However, treating the Amish themselves can be a
real challenge. I ran on a call for a child with a traumatic injury after being kicked by a horse. My partner
and I wanted to fly the child to a nearby hospital, but
the family said ‘no helicopter; just take the patient
to the hospital and let God decide the outcome.’ As
a healthcare provider, sometimes they do tie your
hands as far as treatment and transport go.
James Adams
Via Facebook
I work in northeast Indiana, and we have a large Amish
population. We have a very good relationship with
them, perform occasional safety days for them and
have several medics who travel to Amish schools
with an ambulance to interact with the kids. We have
several EMTs and medics who grew up Amish, which
is helpful for speaking with the young kids who don’t
speak English. As mentioned, there are sometimes
differences in opinions, as far as flying patients (they
strongly prefer not to use the helicopter), and they
definitely don’t call unless things are very serious. The
one thing you can always count on, with the Amish,
though, is that they’re very grateful for our help and
are supportive of what we do. JEMS
Julie Shoemaker
Via Facebook
Amish Perspective
As a former EMT with Lancaster EMS as well as Strasburg
EMS, I’ve worked with several of the Amish EMTs, and I
must say they’re very dedicated and caring for the entire
community—not just their own people. The area that
they cover is a large tourist area, and they work well
Do you have questions, comments or concerns
about recent JEMS or JEMS.com articles? We’d love
to hear from you. E-mail your letters to editor.jems@
elsevier.com or send to 525 B St. Suite 1800, San Diego,
CA 92101, Attn: Allison Moen.
While I was responding to a code orange (a suicidal
psych patient), who had just been struck by a vehicle in
an attempt to take his life after assaulting his mother in
her home, police and sheriff were on scene as my unit
arrived. I’ve done mixed martial arts for a few years, and
when three law enforcement officers and one of my
two partners couldn’t restrain the patient, I fell back on
18
JEMS
MAY 2012
Due to graphic content,
rubbernecking
discretion is advised.
illustration steve berry
Like I was taught, I don’t plan to fight; I plan to end it.
And I’m not referring to irrational, overdose or dementia
patients. I’m referring to the rational patients who might
turn on us one day. Everyone is always happy to see EMS.
Cops are always immediately on hand and helpful, and
happy endings are guaranteed, right? The truth is, you
never know when something might happen. I believe in
doing no harm first and foremost. I also believe in coming home safe and in one piece after every shift.
Heather Gaff Mewis
Via Facebook
19. Comprehensive, Credible, Educational...
JEMS Products
Help You Save Lives.
Jems, Journal of Emergency Medical Services
jems.com Website
With content from writers
who are EMS professionals
in the field, JEMS provides
the information you need
on clinical issues, products
and trends.
Your online connection to the
EMS world, JEMS.com gives
you information on:
• Products
• Jobs
• Patient Care
• Training
• Technology
Available in print or digital
editions!
jems.com eNewsletter
Product Connect
Sign up now for the weekly
JEMS.com eNewsletter.
Get breaking news, articles
and product information
sent right to your computer.
Read it on your time and stay
ahead of the latest news!
4 NEW Webcasts!
Giving you the detailed product
information you need, when
you need it. We collect all the
information from manufacturers
and put it in one place, so it’s
easy for you to find and easy
for you to read.
Go to www.jems.com/ems-products
Register at JEMS.com/webcasts.
Watch
live or in the
archives!
n EMS Strategies for Improving Cardiac Arrest Survival
May 21 2012, at 1 p.m. ET/10 a.m. PT Sponsored by:
n Drug Shortage Action Plans for EMS Sponsored by:
n Are You Bagging the Life Out of Your Patients? Sponsored by:
n Statewide Trauma System Enables Multi-Agency Coordination with
Trauma Centers to Improve Patient Outcomes Sponsored by:
Go to www.JEMS.com
20. PRIORITYUSE
TRAFFIC
NEWS YOU CAN
EMS on the HILL
NAEMT hosts third-annual event
the line of duty; and
he legislation to establish new
T
EMS grant programs; enhance
research initiatives; and promote
high-quality, innovative and costeffective field EMS.
To assist active members in attending EMS on the Hill Day, NAEMT
awarded grants of up to $1,200 each to
four active members.
One of the grant recipients was Jason
Scheiderer, EMT-P, of Indianapolis,
Ind. He’s employed by Indianapolis
EMS and teaches paramedic courses at
Indiana University-Purdue University
Indianapolis. Scheiderer has advocated for local issues, walking the
fine line between concerned taxpayer
and public employee. NAEMT’s state
advocacy coordinator for Indiana,
Scheiderer appreciates NAEMT’s focus
on improving EMS on a grand scale. “Not
getting into local issues like fire department
vs. private EMS providers,” he says.
W. Mike McMichael III, EMT-B, and 2011
NAEMT grant recipient from Delaware,
returns to Washington for the 2012 event.
McMichael says, “I’m tickled to death to be
involved” in this endeavor that “will help
everyone in the country.” Although he
personally knows his representative and
Delaware’s two senators, he liked the opportunity to see them working.
On May 4, 2011, in Washington, D.C., 145
EMS professionals from 39 states and the
District of Columbia and Puerto Rico met
with more than 217 U.S. Senators, House
Representatives and their congressional staff
at the second annual EMS on the Hill Day.
The fourth EMS on the Hill Day is tentatively scheduled for the first week in March
2013. That would coincide with 2013 EMS
Today, so you could attend both on one
plane ticket.
Mark your calendar and watch the NAEMT
site for more details in the months to come.
—Ann-Marie Lindstrom
photo dreamstime.com
L
ook out, Washington, here
comes EMS. Paramedics and
EMTs from across the country went to the hill for the third
time to talk to members of Congress
about what’s important to the EMS
community and its patients.
There’s only so much that can
be done on the local and state levels. Federal funding and guidance
is needed in some areas. And that’s
why we saw the third EMS on the
Hill Day, hosted by the National
Association of Emergency Medical
Technicians (NAEMT).
Legislators have to hear from
their constituents if there’s any
chance of them understanding what’s going on outside of
Washington. EMS providers go to
talk to their representatives and senators about what they see as a non-partisan
issue: providing quality care to their patients.
NAEMT President Connie Meyer, EMTP, EMS captain for Johnson County MedAct in Olathe, Kan., was excited about
this year’s EMS on the Hill Day. She says
they expected 190–200 EMS personnel to
attend—up from 145 in 2011. Something
new this year was a partnership with the
American Ambulance Association (AAA).
AAA participation replaced their regular
lobby day.
EMS on the Hill Day attendees were invited
to participate in AAA’s Reimbursement Task
Force meeting on Tuesday afternoon, March
20, for discussions on reimbursement issues,
healthcare reform, Medicare ambulance relief
and other emergent topics.
Tuesday evening included a pre-visit briefing with the opportunity for attendees to
mingle and see old friends or network with
new contacts.
Wednesday morning, the visits to
Congressional offices began. Armed with
their talking points (more on that below),
EMS professionals met with their representa-
tives and senators or staffs. The meetings not
only gave EMS personnel the chance to speak
of legislature issues that touch them professionally and personally, but they also allowed
the legislators the opportunity to learn more
about EMS. During a previous visit, one staffer
asked, “So you’re not a fire man?”
And the knowledge exchange has already
led to an event that Meyer characterized as
“huge.” What she’s referring to is a request
from a federal legislator for NAEMT input
on a bill being written. An elected official in
Washington came to NAEMT for advice.
While visiting the Congressional offices,
attendees have talking points, supplied by
NAEMT. This year’s issues include the following talking points:
The Medicare Ambulance Access
Preservation Act of 2011 to provide for a
more permanent solution to below-cost
Medicare ambulance reimbursement;
he extension of death and other benT
efits under the Public Safety Officers’
Benefits (PSOB) program to non-profit,
nongovernmental paramedics and
EMTs who die or are severely injured in
For more of the latest EMS news, visit jems.com/news
20
JEMS
MAY 2012
21. photo dreamstime.com
Mardi Gras No
Party for EMS
New Orleans EMS responded to more
than 2,000 calls during a 10-day
period in February.
That’s 67 more than
their
normal
activity. Despite
all the strange
weather across the
country this winter, the increased call volume in New Orleans wasn’t
because of hurricanes or other natural disasters.
It was Mardi Gras—definitely a man-made, and perhaps unnatural, event. Weeks of reveling take their toll on the thousands of
residents and tourists who show up for the 60 Krewe parades and
other celebrations.
Deputy Chief of EMS Ken Bouvier says, “Obviously, there’s a lot of
alcohol poisoning.” Perhaps, not unrelated, there are also falls from
ladders and balconies in the French Quarter.
Bouvier says their transportation fleet included 25 ambulances, six
Fast Cars, an ASAP mini-ambulance, two bicycles and an 18-stretcher
mobile ambulance bus.
The parade route is approximately 60 city blocks, according to
Bouvier. “We try not to cross parades, so we have staff on both sides
of the streets.”
The Red Cross saw about 1,000 patients in its four first aid tents.
The tents were staffed with six to eight volunteers ready to treat such
minor complaints as sprains, foreign objects in the eye or requests for
a Band-Aid. Red Cross first responders also wandered through the
crowds keeping an eye open for anyone in need of medical assistance.
Armed with radios, the first responders called EMS as needed.
Bouvier characterized this year’s Mardi Gras as “well attended”
without violence along the parade route—evidently that’s noteworthy when you talk about Mardi Gras.
Planning
Planning is paramount for a city-wide, three-week celebration.
Bouvier says they start planning for the next year about a week after
Mardi Gras ends. They look at the statistics and reports to see what
worked and what could be improved. For example, the city made
more use of the Red Cross this year, “because it works,” says Bouvier.
The mini ambulance and bike teams are new additions, too.
As Mardi Gras draws near, New Orleans EMS has to make sure it
has enough medications on hand, enough staff ready to work—forget about ever getting time off to enjoy the festivities with your family
or friends—and enough ambulances ready to roll.
Next year’s Mardi Gras will be an enhanced challenge, says
Bouvier. New Orleans hosts Super Bowl XLVII on February 3, 2013,
so the city has decided to split up the Mardi Gras events to bookend
the Super Bowl. That is, there will be a week of Mardi Gras celebration, a week devoted to Super Bowl activities and then another week
of Mardi Gras.
Bouvier says they will be ready. And they’ll all probably be ready
for a long vacation in March. —Ann-Marie Lindstrom
Choose 20 at www.jems.com/rs
www.jems.com
MAY 2012
JEMS
21
22. continued from page 21
QUICK TAKE
T
Debunking HIPAA Myths
he healthcare industry has come a long way since Health Insurance Portability and Accountability Act
(HIPAA) went into effect almost a decade ago. For the most part, EMS providers now have a much better understanding of how HIPAA applies to their day-to-day operations. Nevertheless, many “HIPAA myths”
still exist. Here are some of the top myths in the EMS industry today.
Myth: HIPAA prevents EMS agencies and facilities
from sharing patient information.
All healthcare providers should know that HIPAA permits them to freely
share patient information for treatment-related purposes. That means that
facilities can give EMS providers medical records about patients, and crews
can look at those records for treatment purposes. It doesn’t matter that
another provider created the medical record.
Ambulance services may also provide a copy of their trip reports to
facilities because such practice would also fall under the “treatment”
umbrella. Under HIPAA, “treatment” includes
the provision, coordination and management of
healthcare between providers.
Pro Bono is written by
attorneys Doug Wolfberg,
Ryan Stark and Steve
Wirth of Page, Wolfberg
Wirth LLC, a national
EMS-industry law firm. Visit
the firm’s website at www.
pwwemslaw.com for more
EMS law information.
photo courtesy NEMSMBR
Myth: Law enforcement offi-
EMS providers travel across the country for
the National EMS Memorial Bike Ride.
2012 National
EMS Memorial
Bike Ride
The National EMS Memorial Bike Ride
(NEMSMBR) is gearing up for the 2012 Ride,
with routes beginning in Boston, Mass., or
Paintsville, Ky., on May 19—both finishing in
Alexandria, Va., on May 25.
During the ride, participants will travel
through the states of Massachusetts, Kentucky,
Rhode Island, Connecticut, New York, New
Jersey, Pennsylvania, Maryland and Virginia.
“To see these parts of the United States on
a bicycle is such a unique perspective,” says Tim
Perkins, NEMSMBR public information officer.
“It’s also great to interact with the providers and agencies along the route, not to
mention the reason for the ride: honoring over
30 individuals who have given the ultimate sacrifice providing EMS care,” says Perkins.
Additional rides are scheduled for
Colorado in June and Louisiana in September.
For more information
about the bike ride,
visit www.muddyangels.com.
Many EMS providers believe that if a law
enforcement official asks for information about
a patient, they’re automatically entitled to it.
Although there are circumstances under which
ambulance services may release patient information to law enforcement, there’s no general provision in HIPAA that broadly permits providers to
release patient information to law enforcement.
To the contrary, providers can only give patient information to law enforcement officials under specific
circumstances.
If an ambulance service receives a request for healthcare information from law enforcement, the service
must check to see whether HIPAA contains a specific exception that permits the release of the information.
Some of the more common exceptions include reporting a crime in an emergency or disclosures that are
required by state law (e.g., gunshot wounds and dog bites). Check with your HIPAA privacy officer before you
release information to law enforcement. If you improperly disclose information, you risk violating HIPAA, and
that information might not be allowed to be introduced as evidence because it was improperly obtained.
Myth: It’s OK to post as long as the patient isn’t identified.
EMS providers have a legal and ethical duty to refrain from posting any “protected health information”
(PHI) on the Internet. Most of us know that PHI is anything that could directly identify a patient. However,
what many fail to consider is that some information might reasonably identify a patient, even though it
doesn’t mention a patient by name. The bottom line is that if someone reading the post might be able to
figure out who the patient is, the information might be PHI, and posting it could violate HIPAA.
For example, a post stating, “Was on a pretty crazy trauma on I-95 tonight … that guy had no shot,” might
convey enough information to enable friends or family members of the deceased patient to identify him
because they undoubtedly know about the incident.
Because others can determine the identity of the patient from the limited information provided, this
post improperly divulges PHI. Generally, no legitimate reasons justify posting any information about a
patient on the Internet. Moreover, it’s unethical—and unprofessional—to refer to a patient, in any manner,
on the Internet.
Check out all the upcoming free webcasts JEMS has to offer: www.jems.com/webcasts
22
JEMS
MAY 2012
photo dreamstime.com
cers are automatically entitled to patient information.
24. LEADERSHIP SECTOR
presented by the iafc ems section
by gary ludwig, ms, emt-p
Crisis Management
Rudy Giuliani advocates for managing things, not people
W
e’re familiar with the usual type
of leadership that a manager at
IBM, Bank of America or the corner grocery store shows when managing their
operation and people. Usually these managers mistakenly try to manage people when
they should be leading people. The important thing to remember is that we manage
things and we lead people. We manage budgets,
inventory and fleets.
It’s rare that the manager working at IBM,
Bank of America or the corner grocery store
need to lead people in a crisis. That isn’t true
for the EMS manager. Not only do they have
to lead people under normal everyday conditions, but they also may be asked to show
their leadership during high-intensity events,
such as tornadoes or mass-casualty incidents.
EMS managers may be thrust into a leadership role during an active shooter attack.
The leadership skills that an EMS manager
must exhibit during a crisis are much different from the leadership skills that they use
in their day-to-day operations. In their dayto-day office operations, they have the ability to sit back and use discretionary time to
make a decision. If someone comes into their
office with a problem, the EMS manager has
the luxury of requesting more information,
maybe making some phone calls, sitting on
it overnight or even checking with their boss
before they make a decision.
Unfortunately, that isn’t the case on the
scene of an active shooter or a bus crash.
Sometimes split-second decisions must to be
made. Sometimes decisions have to be made
with limited information. And sometimes
the EMS manager may have to make some
tough decisions that have a direct affect on
someone’s life. The leadership skills that an
EMS manager must show during these critical times are crucial.
Leadership Tips
In my opinion, one of the finest examples
of leadership was former New York City
Mayor Rudolph Giuliani’s management of
24 JEMS
MAY 2012
‘It is in times of
crisis that good
leaders emerge.’
9/11. Don’t forget, the U.S. president was
sheltered away until late in the evening to
protect the head of our federal government.
President Bush wasn’t seen on television; it
was Giuliani who became the face of reassurance on television for the American people.
But 9/11 wasn’t the only time Giuliani was
thrust into a crisis. He routinely showed up
at emergency scenes in New York City.
Giuliani describes four steps for crisis leadership in his book Leadership. “It is in times of
crisis that good leaders emerge,” he says.
He says the first step is to be visible. Giuliani
says, “While mayor, I made it my policy to see
with my own eyes the scene of every crisis so
I could evaluate it firsthand.”1
Who can forget those scenes of Mayor
Giuliani walking on the streets of New York
with his contingent of staff and department
heads while being interviewed by the news
media? EMS managers must respond to
scenes and take charge of their operation.
Many times, they fall into the incident management structure. Although they may not
have overall command of an event,
EMS managers are still responsible for
the medical operations branch.
Giuliani’s second step is to be composed. He writes in his book, “Leaders
have to control their emotions under
pressure. Much of your ability to get people to
do what they have to do is going to depend on
what they perceive when they look at you and
listen to you. They need to see someone who
is stronger than they are, but human, too.”
Many times in my career I’ve seen an incident commander yell or even scream into a
radio. Yelling on the radio or at employees
on a scene, or giving an appearance of being
out of control, is a prescription for crisis—the
situation EMS managers are trying to control.
Giuliani’s third step is to be vocal. He
writes, “I had to communicate with the public
to do whatever I could to calm people down
and contribute to an orderly and safe evacuation [of lower Manhattan].”
EMS managers must demonstrate the
same trait during a high-intensity event.
You need to be able to give people firm
directions and instructions. You need to
give your employees or others clear and
concise instructions or action steps.
Giuliani’s fourth step to crisis leadership
is to be resilient. Giuliani describes himself
as an optimist. With his words during some
of his press conferences about 9/11, he gave
Americans hope that they would meet this
challenge and overcome it.
EMS managers must also show the same
resiliency. They demonstrate through actions
and words that whatever the challenge that
the EMS organization and its employees are
facing, they’ll be able to deal with it.
And, most importantly, always remember
there are times to demonstrate everyday leadership and times during emergencies that you
have to demonstrate true leadership skills. JEMS
References
1. Giuliani R: Leadership. Hyperion: New York, 2002.
Gary Ludwig, MS, EMT-P, is a deputy fire chief
with the Memphis (Tenn.) Fire Department.
He has 34 years of fire and rescue experience. He’s chair of the EMS Section for the
International Association of Fire Chiefs and
can be reached at www.garyludwig.com.
27. photo istockphoto.com
Management Focus
The medical director units that arrive
on-scene with a physician are especially
beneficial during mass casualty incidents.
Emergency physicians assist their prehospital counterparts
By Richard Huff, NREMT-B
I
f a call for a mass casualty incident (MCI)
goes out in northern New Jersey, there’s
a good chance James Pruden, MD, the medical director for emergency preparedness
at St. Joseph’s Regional Medical Center, is
going for a ride.
Pruden is part of a breed of physicians
who are just as comfortable working outside
of the confines of an emergency department
(ED) as they are in the field—where they can
be more helpful controlling a scene.
“There’s a subset of physicians, wild and
crazy guys, who get that surge and pleasure
being out there in the environment,” says
Pruden, who heads up St. Joseph’s Emergency Physician Response Vehicle program, MD-2.
The St. Joseph’s program, which is part
of the New Jersey EMS Task Force system, is
used to respond to everything from school
bus rollovers, to fires and planned events
throughout the region.
The parameters for the units being dispatched are wide open, but the common
thread is that the doctors responding are different from their hospital-bound brethren.
“It’s not just about having an emergency physician,” says Scott Matin, vice
president of Mobile Health Services at the
Monmouth Ocean Hospital Services Corporation (MONOC), which also launched
mobile physician unit MD-1 in January.
MONOC’s MD-1 unit is headed by Mark
Merlin, MD, a new member of MONOC’s
Medical Advisory Board, chair of the EMS/
Disaster Medicine Fellowship at Newark
Beth Israel Medical Center and medical
director of the New Jersey EMS Task Force.
MD-1 is stationed with Merlin or a member
of his team.
“It’s about having someone with emergency experience. It is different doing
something in the emergency room than it
is having to do it in the field. You’re not on
a table, but in the back of [a] crashed upside
down vehicle,” says Matin.
And that’s where the mobile physicians’
units come into play, especially at times
when there may be an MCI or some other
incident in which the scene could use a
physician on hand.
In some ways, the MD units are a
“force multiplier,” says Robert J. Bertollo,
MICP, LRCP, MBA, the program manager of Life Support Education and Emergency Response Operations for St. Joseph’s
Regional Medical Center.
St. Joseph’s Regional Medical Center has
operated an MD unit for two years that was
funded through the Urban Areas Security
Initiative. Pruden recalls a scenario a few
years ago—before MD-2 existed—during
which employees at a local factory were
overcome by a chemical odor that traveled through the building. There were hundreds of potential patients involved, and 50
www.jems.com
MAY 2012
JEMS
27
28. Extra Set of Hands
continued from page 27
ended up being transported to local EDs.
“What you can do is send the physician to the site, where you then
have the ability to express people on the scene,” Pruden says.
Triage and treatment protocols could have been decided on the
scene of the factory incident, he says, altering the volume of patients
sent to local hospitals.
MD Units Use
There has been an increase in the use of MD units in the field around
the country in recent years. For example, besides the units in New
Jersey and Erie County, New York, has a Specialized Medical Assistance Response Team, which is a volunteer public health emergency
response organization that makes physician response available
around the clock.
For the most part, the MD units are similar. They’re staffed by
physicians like Pruden, who enjoy the challenge of working at an
emergency scene. Typically, the medical teams operate out of nontransport-type sports utility vehicles that mimic paramedic vehicles—although without the required depth of supplies. Some units
include equipment for on-scene surgical procedures.
The initial concept for MD vehicles in EMS responses was for the
more serious patient scenarios in which extrication may severely
cut into the golden hour and reduce survivability. It’s safe to say,
In some ways, the MD units are a
‘force multiplier.’
however, the parameters for use are evolving. Although relatively
new in New Jersey, the greatest use so far has been for MCIs and
pre-planned events, such as major festival concerts for which a high
range of injury is likely.
“Its real worth is when there’s a physician on scene and in a medical control capability,” says Bertollo. In those cases, the specially
trained doctors can increase the volume of patients handled on
scene by taking medical control.
“When it gets to the point where you need that, a doctor can make
multiple decisions,” Bertollo says.
“If you are at the scene, you can identify and quickly establish
symptom protocols,” Pruden adds.
The Monmouth Ocean Hospital Service Corporation unit
wouldn’t respond to the typical EMS call, but rather come into play
for cases in which someone is trapped for an extended amount of
time, or when there might be a need for an emergency amputation
to free the patient.
“These are going to be ones where a half-hour response time still
means you’re going to make it to the scene,” Matin says.
Protocol
At St. Joseph’s, the response parameters for the MD unit have been
pretty broad, Bertollo says, and often left to an on-scene agency to
request the team. When the program was launched, he explains, the
folks at St. Joseph’s visited regional EMS providers to familiarize
them with the operation.
Choose 23 at www.jems.com/rs
28
JEMS
MAY 2012
29. “You need a physician because you’ve transcended the ability of
the EMTs or paramedics on scene,” he says. “We’ve had multiple
patients at fire scenes, industrial accidents ... and we’ve certainly dispatched during floods,” he adds. “Also, if there are specialty things,
like a shooting or multiple-patient pediatric calls.”
There will be more use of the unit in mass casualty situations
than a physician strapping on a surgical kit to do an on-scene amputation or blood transfusion, says Bertollo. The dispatch operation
serving St. Joseph’s has put a system into place: When something
on scene seems unusual, a call goes out to the five physicians on the
MD-2 team.
“Basically, what we’ve said is if you get into a circumstance where
you find something unique or strange looking and the medics say,
‘we wish we had a doc out here,’ give us a call,” Pruden says.
Doing so, of course, gives the physicians in the program real-time
exposure with the frontline emergency responders they normally
wouldn’t see with any regularity, making everyone more comfortable in future scenarios. Likewise, it also gives the physicians experience in situations that are dissimilar from routine ED settings.
And it also expands the program beyond simply preparing EMS
providers to respond to “the big one,” adds Pruden.
There are benefits to the mobile physician teams beyond
responses, too. The folks at MONOC expect to use Merlin and his
team in educational situations and drills.
“What’s nice about this program is, we hope in the end there is not
a lot a huge need for it,” Matin says. “There are added benefits being
involved with this program. We do a tremendous amount of education. Having that number of physicians at hand is a fantastic thing.”
EMS Interaction
Having a higher medical authority on the scene of an EMS call
does raise the potential for conflicts between providers. Matin says
he understands there could be concerns about how EMS providers react in the field to the arrival of a physician on the scene, but it
shouldn’t be a problem in this case.
“These doctors are going to be coming out on special scenes,” he
says. “I can tell you the medics will be glad they’re there.”
Bertollo agrees, “They’ve integrated well. The physicians that have
staffed those responses have known from the outset they’ve wanted
to be an integrated player. We’re here to augment and lend support.”
Pruden goes a step further, noting the goals of the MD-2 unit are
similar to why he loves disaster responses.
“It’s the unity of purpose,” he says. “In an event, when you’re
responding to some critical event, you and other human beings have
the same goal, to help people, to get a response, to turn this thing
into the most positive outcome you can make. Frequently, those
events suppressed ulterior motives. It’s amazing to work in an environment where everybody has the same goal. It’s an incredible rush
to be engaged with that kind of mindset where people are working
together.” JEMS
Richard Huff, NREMT-B, is an active member and the former chief of the Atlantic
Highlands (N.J.) First Aid Safety Squad. He’s a CPR, CEVO and first aid instructor and
multi-dimensional EMS educator. He’s also an award-winning journalist and author.
Choose 24 at www.jems.com/rs
www.jems.com
MAY 2012
JEMS
29
30. TRICKSour patients ourselves
OF THE TRADE
caring for
by Thom Dick, EMT-P
Numbers
Reflections on the value of one
30
JEMS
MAY 2012
Photo istockphoto.com
I
don’t think you can quantify everything
that’s important in life. But in all of the
science on which emergency medicine
has come to depend, we never seem to give
up trying.
Think for a moment. We use a numeric
score to rate people’s pain. (I don’t think it
tells us a dang thing.) We use endless scales
to measure the concentration of ions in their
body fluids, the physical pressure of the
blood in their vascular systems, the color
of their urine, and their heart and respiratory rates. We use scales to assess the sizes
of their pupils and describe the shapes of
their upper airways. We use a trauma score
to predict their survival after they get hurt,
and another scale to describe the severity
of their burns. We imprint depth scales on
the tubes we insert in their orifices. We even
use numeric gradients during our runs to
express the urgency of our responses to
their emergencies.
We frame our lives in the same way, LifeSaver. A while back, my hometown’s pro
football team (the Broncos) braced itself to
take on the New England Patriots in a divisional championship game. The Broncos
were no better than mediocre this year, but
they had supposedly earned a shot at the
Pats by beating the Steelers a week earlier, in
the first few seconds of overtime. The media
and the Bronco fans celebrated the win;
although, few would have blamed the Steeler
fans for believing they were robbed. The final
score was 29–23.
In reality, there was only the barest
margin of difference between the play of
those two teams, and an objective observer
would probably have awarded the win to
Pittsburgh. In addition, the NFL’s history
won’t reflect the fact that Pittsburgh’s great
quarterback, Ben Roethlisberger, played the
whole game on a painful, unstable ankle.
We seem obsessed with the numbers in
our lives. We’ve developed maps to tell us
the depths of the ocean, as well as its salinity, its temperature and how much water it
Our patients are much more than the numbers of their blood pressure reading or their pH level;
they’re individuals.
contains. We assess the effects of the wastes
we pour into it by guessing how many living
organisms disappear afterward. (No doubt
some of us believe there are acceptable numbers of those, too, even if we can’t possibly
count them all.)
We’ve developed systems to help us enumerate the stars, assess their color, brightness, size and mass, and measure how far
they are from us (almost as though we still
believe they revolve around us). We think
we know the volume of the vast space they
inhabit (even if it’s so great, we can’t comprehend it). We’ve envisioned ourselves at the
tippy-top of the hierarchy of all life, based
on the complexity of our cognitive thought
processes. Scholars have attempted since the
fifth century to describe the value of nothing.
(What a surprise: We’ve assigned a number
to that, too.)
We even rate human intelligence using
a numerical value. We call it IQ, for intelligence quotient. We discuss people in terms
of their IQs, as well as their age, height,
weight, body-mass index, annual income,
and belt and neck sizes (as though their
dimensions actually help us to understand
anything about them).
The business of helping people in
crisis is a lot bigger than the stuff
we can measure. Measurements are
simple routines, each of which typically reveals no more than a single
answer to a simple question. What’s
the blood pressure? What’s the blood glu-
cose? What’s the pH?
It’s important to respect what those
numbers tell us, but only as puzzle pieces.
Whatever we do, we need to be much more
focused instead on a prime number we
call “one.”
Serving people is all about individuals.
Taking care of them requires a willingness
to admit that we don’t know much about
them. But we have a persistent commitment
to observe, question, examine and think. In
emergency situations, we sometimes need
to do all of those things at warp speed. (If
anybody ever told you this EMS stuff would
be easy, they altered the truth.)
Next time you kneel in front of somebody
you don’t know or sit beside someone in that
ambulance of yours, look them straight in the
eye. No matter how ordinary they seem, how
ugly or even unpleasant, ask for their name.
And use it. And make sure there’s no doubt
in their mind about one thing: While they’re
with you, they’re important. What they say
matters. And how they feel is essential. Not
just any old person has the talent or the desire
to do that. Those who do are called caregivers.
Are you one of those? If so, you really are
special. JEMS
Thom Dick has been involved in EMS for
42 years, 23 of them as a full-time EMT and
paramedic in San Diego County. He’s currently
the quality care coordinator for Platte Valley
Ambulance, a hospital-based 9-1-1 system in
Brighton, Colo. Contact him at boxcar_414@yahoo.com.
31. Choose 25 at www.jems.com/rs
Choose 26 at www.jems.com/rs
32. CASE OF THE MONTH
DILEMMAS IN DAY-TO-DAY CARE
BY Jeff Westin, MD; Pat Songer, NREMT-P, ASM; Kelly
Buchanan, MD; Loren Gorosh, MD; Ryan Hodnick, DO;
Bryan E. Bledsoe, DO, FACEP, FAAEM
Miracle in the Desert
Cardiac case at remote Burning Man event presents challenges
Remote Care
On the final day of the Burning Man event,
EMS is summoned to a chest pain call
in a trailer within the encampment. On
arrival, paramedics find a 60-year-old male
in acute distress.
He’s pale and diaphoretic and in extremis.
The patient describes the pain as “tearing”
Photo courtesy Bryan Bledsoe
B
urning Man is a massive event held
around every Labor Day in the Black
Rock desert in northwestern Nevada.
The encampment is an official city called
Black Rock City, and although it exists for
only a week or so each year, it becomes
the third-largest city in Nevada. The event
attracts in excess of 50,000 attendees.
The purpose of Burning Man is radical
self-expression in various art forms. It’s
truly a one-of-a-kind event. Black Rock
City operates as a functional geopolitical
entity with fire, police and EMS systems.
Each is dispatched from a manned communications center that’s constructed and
deconstructed annually.
In 2011, Humboldt General Hospital
EMS in Winnemucca was contracted to
provide medical care for Burning Man.
Medical care included a fully staffed and
operational EMS system, as well as a field
hospital called Rampart General and two
BLS aid centers.
A total of 2,307 patients were treated.
Three-hundred and eighty-two requests for
ambulances were made, with 185 patients
being transported to Rampart General.
Only 33 patients were transported out of
the desert for care. The following highlights one of those cases that took place
during the event.
Burning Man, an elaborate weeklong festival in the Nevada desert, presents unique challenges to
EMS providers.
and can’t get into a comfortable position.
The EMS crew extricates him from his trailer
and moves him to the awaiting ambulance
for a more detailed assessment.
He becomes unresponsive shortly
after they place him in the ambulance.
Paramedics check his pulse, take a quick
look at the monitor, and note the patient
is in a non-perfusing v tach. On a hunch,
they administer a precordial thump, and
it works. The patient converts to a sinus
rhythm. He’s transported to Rampart
General in Black Rock City.
Once the patient arrives at the field hospital, the emergency staff rapidly assesses
him. He’s alert and oriented, but his blood
pressure is undetectable. He’s writhing in
pain on the stretcher. IV fluids are given,
and his blood pressure is finally detectable
at a systolic pressure of 72 mmHg and then
up to 76 mmHg. He remains mildly tachycardic. He receives IV fentanyl for pain.
Rampart General has X-ray capabilities and
a stat chest X-ray is obtained. The emergency physician notes that the mediastinum is wide at 10.5 cm—consistent with
a thoracic aortic aneurysm and dissection.
A medical helicopter is summoned and the
patient is closely monitored and stabilized
by the emergency staff.
As soon as the helicopter arrives,
the patient is moved to the aircraft and
transported to a major medical center
about 150 miles away. Once he arrives, he
undergoes a computed tomography angiogram (CTA) that confirms the suspected
aortic dissection.
The patient is emergently taken to surgery where the aneurysm is repaired. The
operation is successful, and the patient is
A case from university medical center in LAs VEGAS
32
JEMS
MAY 2012
33. moved to the intensive care unit (ICU).
Following surgery, the patient suffers a second cardiac arrest
and is taken to the cardiac catheterization lab for evaluation and
subsequent stenting of a coronary artery lesion. He’s returned to
the ICU and remains stable. He’s discharged home with appropriate provisions for follow-up. Despite his ordeal, he’s already planning his next trip to Burning Man.
Discussion
First, this is not a true “case from University Medical Center”
because it didn’t happen at UMC. However, emergency physicians, emergency medicine residents and medical students from
the University of Nevada School of Medicine provided much of
the medical care at Burning Man. As you can tell, this patient had
all the cards stacked against him. He had a critical thoracic aortic
dissection, and he was in the middle of a Nevada desert more than
150 miles from a medical facility with cardiothoracic surgery capabilities. Furthermore, he suffered a cardiac arrest. Yet despite all of
this, he survived.
Thoracic aortic aneurysms and dissections are life-threatening
conditions that affect the thoracic portions of the aorta. An
aneurysm is a dilation of an artery greater than 50% of its normal diameter. They’re classified based on the region of the aorta
affected (e.g., ascending aortic, aortic arch, descending aortic and
thoracoabdominal), and are at risk for rupture.
A dissection results from a tear in the interior lining of the aorta
(the tunica intima). This tear, referred to as an intimal tear, causes the
layers of the aortic wall to separate thus forming a false lumen. The
pressure from the blood within the aorta causes the false lumen to
expand, or dissect.
As the dissection progresses, blood flow to various blood vessels is affected, causing ischemia to the tissues they supply (e.g.,
the coronary arteries and spinal cord). Thoracic aneurysms most
commonly occur in persons older than age 65. Death from a ruptured aneurysm is typically one of the top 10–20 causes of death
annually. The incidence of thoracic aneurysmal rupture is approximately 3.5 per 100,000 persons.1
Patients who develop cardiac arrest from a thoracic aneurysmal dissection rarely survive. Furthermore, resuscitation with a
precordial thump is even less common.2 Hypotension is common,
and hypertension should be avoided. This patient received enough
fluids to restore perfusion as determined by monitoring his mental status and a maintaining a systolic blood pressure between
76–78 mmHg.
Consideration was given to adding vasopressors, but because
dissection was suspected, they weren’t administered. A thoracic
aortic dissection is characterized by widening of the mediastinum
on chest X-ray. Fortunately, limited X-ray capabilities were available at Rampart General. The diagnosis was later confirmed by a
CTA at the receiving hospital.
Teaching Points
It’s often difficult to diagnosis aortic dissection, either thoracic or
abdominal, in the prehospital setting. Because of this, EMS providers must have a high index of suspicion when patients present with
signs and symptoms consistent with thoracic aortic dissection.
The most common presenting sign is pain—either in the chest or
Choose 27 at www.jems.com/rs
www.jems.com
MAY 2012
JEMS
33
35. CASE OF THE MONTH
continued from page 33
between the scapulae in the upper back. With large aneurysms,
the superior vena cava can be compressed, causing distended neck
veins. A murmur may be heard. Sometimes hoarseness, cough
and wheezing may be present. In other instances, such as this one,
shock and cardiac arrest may be present.
So much of quality EMS is identifying injuries and illness in the
field, recognizing the potential severity and ensuring the patient is
rapidly transported to an appropriate medical facility.
The concerns of EMS crews and a presumptive field diagnosis can also aid emergency department personnel in directing
appropriate resources to critically ill or injured patients. Quality
emergency physicians will listen to the concerns of field crews and
react accordingly.
Summary
This was a miraculous case that illustrates the importance of seamless interaction between field EMS crews and physicians. First,
this case occurred in one of the most austere and hostile environments imaginable. Next, it included a patient who was resuscitated
from pulseless v tach with a precordial thump performed by a
paramedic crew. The patient was subsequently evaluated and
diagnosed with a thoracic aorta dissection by medical staff in a
tent (with a diagnosis made by plain chest X-ray) and emergently
transported 150 miles to a hospital where successful surgery was
carried out.
It truly was a “perfect storm,” or perhaps, it was the general
goodwill and spirit of Burning Man. Or maybe those crystals that
were everywhere actually worked. JEMS
Jeff Westin, MD, was a third-year emergency medicine resident at the University
of Nevada School of Medicine. He’s an attending emergency physician for KaiserPermanente in Portland, Ore. He can be contacted at jeffwestin@yahoo.com.
Pat Songer, NREMT-P, ASM, is director of EMS at Humboldt General Hospital
EMS. He can be contacted at psonger@hghospital.ws.
Kelly Buchanan, MD, is an EMS fellow at the University of Nevada School of
Medicine. She can be contacted at shorti3181@gmail.com.
Loren Gorosh, MD, is a third-year emergency medicine resident
at the University of Nevada School of Medicine. He can be contacted at
lorengorosh@gmail.com.
Ryan Hodnick, DO, is a second-year emergency medicine resident
at the University of Nevada School of Medicine. He can be contacted at
lasvegas.em@gmail.com.
Bryan Bledsoe, DO, FACEP, FAAEM, is professor of emergency medicine at
the University of Nevada School of Medicine and director of the EMS Fellowship
Program. He is also the medical director for Burning Man. He can be contacted at
bbledsoe@me.com.
References
1. Rogers RL, McCormack R. Aortic disasters. Emerg Med Clin North Am.
2004;22(4):887–908.
2. Haman L, Parizek P, Vojacek J. Precordial thump efficacy in termination of
induced ventricular arrhythmias. Resuscitation. 2009;80(1):14–16.
Choose 29 at www.jems.com/rs
www.jems.com
MAY 2012
JEMS
35
36. RESEARCH REVIEW ems
What current studies mean to
by David Page, MS, NREMT-P
Gender Matters
Study compares cardiac care for male vs. female patients
Photo istockphoto.com
Aguilar SA, Patel M, Castillo E, et al. Gender differences
in scene time, transport time, and total scene to hospital arrival time determined by the use of a prehospital
electrocardiogram in patients with complaint of chest
pain. J Emerg Med. 2012; Feb 15. [Epub ahead of print].
T
hese authors retrospectively analyzed
San Diego EMS charts, measuring the
effect of prehospital 12-lead ECGs on scene
times. Out of 21,742 chest pain calls, no significant scene time increases or differences
were found between patients with and
without ST-elevation myocardial infarction
(STEMI). This is nothing new; this has been
studied many times. The researchers did,
however, find that in STEMI cases, male
patients had an average of 17-minute scene
times vs. females, who had 20-minute scene
times. This delay is then projected to a possible increase of 0.25–1.6% greater mortality.
This study adds to a growing body of
literature showing that women experiencing
acute coronary syndromes receive delayed
diagnosis and care. Possible explanations
could include atypical presentations, delayed
symptoms or comorbidities. I’ll add my own
observation that performing prehospital
12-leads on women involves a certain need
for tact and social privacy that may cause a
delay. In any case, now that we are aware of
it … let’s all try to speed up identification and
care for women having STEMIs.
Waldron R, Finalle C, Tsang J, et al. Effect of gender on
prehospital refusal of medical aid. J Emerg Med. 2012;
Feb 9. [Epub ahead of print].
I
t shouldn’t be any news that patient refusals
often end in adverse outcomes and continue to be a problem for EMS. I applaud
these authors for discovering a new angle
to this issue. This New York City project
retrospectively reviewed one year’s worth
of patient-care reports for a single hospitalbased ambulance service. The staff at this
service is made up of 82 EMTs and paramedics, with 67 men (82%) and 15 women (18%).
36
JEMS
MAY 2012
Study evaluated IM vs. IV treatment.
Out of 19,455 total patient encounters, 238
refusals were documented. (If this is accurate,
congratulations are due on a 1.2% refusal
rate. This is one of the lowest ever reported in
recent literature).
Although most of the refusals came during the evening tour, no correlation was
found to it being in the beginning or near
the end of the crew’s shift. The authors did,
however, discover that crews composed of
two male providers were four times more
likely to have an encounter end in a refusal
when compared to a crew that had one or
both female crew members.
In the discussion, the authors note
that differences in communication styles
between genders may lead to perceptions
of behaviors demonstrating greater care by
female healthcare providers.
I Treatment of seizures I
Silbergleit R, Durkalski V, Lowenstein D, et al.
Intramuscular versus intravenous therapy for prehospital status epilepticus. N Engl J Med. 2012;366(7):591–600.
T
he much anticipated results from the
Rapid Anticonvulsant Medication Prior
to Arrival Trial (RAMPART) study were
published in February in the New England
Journal of Medicine. The study’s main objective
was to show that prehospital intramuscular
(IM) midazolam (10 mg) was just as good as
the in-hospital standard of care: IV lorazepam (4 mg) for status epilepticus.
Because lorazepam has a short shelf life
when it’s stored un-refrigerated, most EMS
systems find it costly and impractical to
carry. Midazolam is widely used, but it
hasn’t been studied well in the prehospital
environment. This landmark prehospital
study will likely be remembered more for its
rigorous scientific methods rather than for
the actual results. It’s a great example of the
“gold standard” of research: double-blinded,
prospective, randomized studies with great
follow through to hospital discharge. The
authors used some innovative and groundbreaking strategies to overcome the usual
hurdles that make prehospital research
so difficult.
First, the details: RAMPART involved
4,314 paramedics from 33 EMS agencies
and 79 receiving hospitals across the U.S.
They enrolled 893 patients and randomly
assigned them to either the midazolam or
the lorazepam group. Neither the patient,
the paramedic nor the receiving hospital
were aware of what medication was administered. The results: IM midazolam stopped
the seizure before hospital arrival 73.4%
of the time while IV lorazepam was 63.4%
effective. They conclude that midazolam is
safe and effective.
Although IV lorazepam had a more rapid
onset, establishing an IV in a seizing patient
was widely variable. Thanks to accurate
time stamps, this study clearly proves that
auto-injectors allow for rapid administration of medications and faster seizure cessation—even if the IM medication is slower
to take effect. Patients who received midazolam were also hospitalized less often and
required fewer intubations.
Now for the unique components that
make this a landmark study. The authors
used a special box that contained both an
auto-injector and the IV medication. The
paramedics were blinded to which treatment they were administering by having
them give all patients an IM shot first, then
starting an IV and giving everyone an IV
bolus. All the auto-injectors and syringes
looked the same, so it was impossible to tell
which had active medication.
37. I glossary I
Placebo: Simulated but ineffective or inert
medication replacement, such as giving injecting
saline instead giving an actual medication.
If the box contained “active” midazolam
auto-injectors, then the IV bolus was a placebo and vice versa. If the box had “active”
lorazepam IV bolus, then the auto-injector was a placebo. This is clever because
many studies have shown that providers
will go to great lengths (even tasting the
two medications) to uncover which is the
“active” medication. This often destroys the
randomization process that is so critical
to research.
Another interesting technique was the
inclusion of an automatic, time-stamped
voice recorder that was activated as soon
as the box was opened. Most studies try
to use the notoriously inaccurate times on
the patient-care report or have providers
fill out an extra piece of paper with study
information—or sometimes they even have
to be interviewed by telephone after the fact.
The paramedics in this study could simply
say what was happening, such as the “IM
shot has been given” and “the seizure has
stopped.” The recordings were later analyzed
and the accurate time stamp extracted.
Note that Seattle’s Medic One program
has measured improvements objectively
for decades with voice recordings for
cardiac arrest patients. This system provides valuable feedback, which the crews
look forward to hearing to help measure
improvements objectively. The technique,
however, is dependent on a cumbersome
ECG monitor add-on, and it unfortunately
hasn’t caught on with the rest of us. It’s
too bad we appear to be more afraid of
recording our errors than we are motivated
to learn from them, and eventually save
more lives. Congratulations to RAMPART
for incorporating state-of-the-art recording
boxes to get accurate data. JEMS
VISIT OGSI at Booth 600
at Disaster Relief
Recovery Expo
Oxygen Generating Systems Intl. / www.ogsi.com / Toll Free 800-414-6474
814 Wurlitzer Drive, North Tonawanda, NY 14120 / jems@ogsi.com / Phone 716-564-5165
Choose 30 at www.jems.com/rs
Visit www.pcrfpodcast.org for
audio commentary.
David Page, MS, NREMT-P, is an educator
at Inver Hills Community College and a
paramedic at Allina EMS in Minneapolis/
St. Paul. He’s a member of the Board of
Advisors of the Prehospital Care Research
Forum. Send him feedback at dpage@ehs.net.
Choose 31 at www.jems.com/rs
www.jems.com
MAY 2012
JEMS
37
39. Law enforcement officers make major
impact as initial care providers
By David Kleinman, NREMT-P Tammy Kastre, MD
I
Photo Matthew Strauss
t was an otherwise quiet morning
in Pima County, Ariz., when, at
10:11 a.m. on Jan. 8, 2011, the Pima
County Sheriff’s Department received
a 9-1-1 call advising of a shooting in
progress at a local shopping center.
During the next 20 minutes, details of
a horrific and historic scene unfolded,
despite the lone shooter being taken
into custody within five minutes of
the original 9-1-1 call.
Before it was all over, that isolated
shooter had fired 30 rounds into a
crowd gathered for the Congress on
Your Corner event with Congresswoman Gabrielle Giffords (D-Ariz.)
outside a busy Safeway grocery store
Officers who are prepared to provide care during
active shooter and hostage situations can be an
asset to EMS.
www.jems.com
MAY 2012
JEMS
39
40. Beyond the Tape
continued from page 39
40
JEMS
MAY 2012
Afghanistan war zones to be the key factor in
preventing death from severe hemorrhage.
Emergency department (ED) physicians
and trauma surgeons from Tucson’s level
one trauma center University Medical Center acknowledge that the quick actions of
the Pima County Sheriff Department deputies and their specialized training and EMS
equipment resulted in decreased hemorrhage, improved vital signs and less need for
shock resuscitation for multiple victims.
Initial First Responders
Photo ASSOCIATED PRESS/ James Palka
It’s essential that treatment begin immediately and patients be transported expeditiously in accordance to the severity of their
injuries. And even in an urban environment,
the time it takes for EMS to arrive on scene
can mean the difference between life and
death for the wounded. Too often the first
responder is a law enforcement officer faced
with a tactical situation of providing a law
enforcement function that must quickly
transition into providing first care to civilians or a fellow officer.
The Safeway shooting happened in a geographic location in Pima County that’s readily served by multiple paramedic units from
three large fire departments. But it’s conceivable that this same scenario could occur
with one or more of the following situational complications:
xtended EMS unit response to a rural
E
or remote setting;
First responders work together on Jan. 8, 2011, at the Safeway where the active shooter event happened.
Photo ASSOCIATED PRESS/ Matt York
on the outskirts of Tucson. Facing the arriving deputies were 19 injured and/or dying
people all in close proximity. Luckily, they
had trained for such situations. Is your
department prepared to receive a 9-1-1 call
like this?
The Northwest Fire Rescue District
(NWFRD) serves the suburban area of Tucson where the mass shooting occurred.
A NWFRD paramedic rescue ambulance
and three ground ambulances from Southwest Ambulance were dispatched based
on the initial information received by dispatch from the initial 9-1-1 call. Three ALS
engines, a ladder company and EMS Captain and Battalion Chief (BC) Lane Spalla
also responded on the first-alarm MCI
response. Three medical helicopters were
also placed on standby based on the scope
of the incident.
Although the first EMS/fire units arrived
on scene in just five minutes, they were held
off in a safe staging area by law enforcement until 10:23 a.m., when the scene was
declared safe for entry.
This scene was also different from many
other active-shooter mass casualty incidents
(MCIs) because the arriving deputies were
all trained in MCI and advanced care procedures that enabled them to play a major role
in the treatment and survival of the multiple
critically wounded patients who were inside
the incident hot zone prior to the secured
arrival of fire and EMS responders.
In the critical minutes of an incident
involving gunfire and the need to secure
the scene, where patients had the potential
to exsanguinate, the deputies arriving on
scene were armed with special emergency
care packs that were strategically positioned
behind the headrest of each patrol vehicle
for easy access and deployment.
During the 47 minutes that deputies were
with the injured at the scene, they treated 10
of the 19 injured patients. They controlled
bleeding, provided rescue breathing and
chest compressions, deployed hemostatic
agents, bandaged numerous wounds, and
assisted citizens and congressional staffers
in the care of the injured.
The first seven patients were triaged,
treated and transported from the scene by
10:35 a.m. All were transported by 11:01 a.m.
The early combat and control of hemorrhage before the onset of shock has been
proven by the military in the Iraq and
Emergency personnel work together at the scene where Rep. Gabrielle Giffords, D-Ariz., and others were shot.
41. Choose 32 at www.jems.com/rs
Choose 33 at www.jems.com/rs
42. Beyond the Tape
continued from page 40
First Five Minutes Training
The concept of training law enforcement officers in initial care and providing them with
special medical kits isn’t new. This is a concept
that has been used by the U.S. Secret Service
for decades, with special kits immediately
available to each agent and all agents familiar
with the items in the kit. However, the First
Five Minutes program is one of the first in
which the care provided by officers before EMS
arrival has been lauded as having saved several
patients. The four-hour First Five Minutes training includes the following elements:
Scene safety and orientation components,
including familiarity with area fire and EMS
agencies and services.
The capabilities of local hospitals and the
availability of helicopter rescue.
Body substance isolation (BSI) and realworld applications.
Assessment of circulation, airway and
breathing. This includes methods to establish and maintain an open airway, as well as
how to provide rescue breathing and continuous compression resuscitation (CCR).
How to contact an injured officer.
When and how to remove body armor.
They also learn a 90-second assessment of the
situation and patient medical conditions with
primary focus on hemorrhage control maneuvers and identification of shock. At the end of
each assessment, deputies are encouraged to
make transport decisions: Do they stay at the
scene and wait for EMS, or do they transport the
wounded rapidly via police or private vehicles?
For hands-on training, the deputies participated in a skills lab that includes the use of the
emergency compression bandages, hemostatic
combat gauze, chest seals and tourniquets.
A Pima County Sheriff’s Department deputy
uses trauma shears during the First Five
Minutes training program.
42
JEMS
MAY 2012
significantly affect the well-being of the
wounded, because the EMS provider would
be markedly delayed in arrival and their
ability to provide essential emergency care.
Early Involvement
In a 2007 study published in Prehospital and
Disaster Medicine, the authors noted, “No
widely accepted, specialized medical training exists for police officers confronted with
medical emergencies while under conditions of active threat.”1
Given the knowledge’ acquired from
historical and modern battle, culminating in the trauma combat casualty care
(TCCC) guidelines, we know the following are causes of preventable death on
the battlefield:
Hemorrhage from extremity wounds;
ension pneumothorax; and
T
Airway compromise.
Each of these conditions can be managed early and effectively using relatively
simple techniques and minimal equipment. Unfortunately these techniques and
equipment are rarely taught to law enforcement officers.
Even in an urban environment, the time
it takes for EMS to arrive on scene can mean
the difference between life and death for the
wounded. Law enforcement personnel routinely are the first arriving responders to
arrive at tactical situations. They are also
often the first to arrive at such mass casualty
situations as major traffic collisions involving multiple patients.
At tactical incidents, officers are often
faced with the challenge of initiating law
enforcement functions and almost simultaneously ensuring that needed care is started
on critically injured fellow officers and
civilians.
Special weapons and tactics (SWAT)
teams have long understood how important it is to have paramedics imbedded in
their teams, immediately available for any
medical need and tactically trained and
aware of how to react and respond in a hostile or active shooter environment. Tactical
EMS (TEMS) providers can readily address
airway, breathing and circulation problems
that create an urgency that transcends the
response times of most staged civilian medical assistance units.
Although it’s not always practical for
law enforcement agencies to employ paramedics to work in the field with officers,
much can be done to train police officers
to care for themselves, their colleagues and
other patients.
Tactical Paramedic Training
In the spring of 2009, the leadership of the
Pima County Sheriff’s Department recognizing the need for global training for all
staff with “feet on the street.” They took
Photo Courtesy David Kleinman
MS resources committed on other
E
high-priority calls and delayed in
response or arrival;
raffic congestion that delays or proT
hibits EMS access to a scene;
n unsafe scene that doesn’t allow
A
fire and EMS providers to approach
immediately.
Any of these complications can
43. Photo Matthew Strauss
Photo Matthew Strauss
elements of TCCC and results from the
research done by Valor Project and created
the First Five Minutes, a tactical emergency
medical training program that was rolled
out to all deputies during annual advanced
officer training. This specialized EMS and
law enforcement training program was
developed with assistance from Richard
Carmona, MD, MPH, the 17th U.S. surgeon
general and former Pima County Sheriff’s
Department SWAT team leader and medical director.
Although the First Five Minutes program
isn’t the first medical training course taught
to Pima County sheriff’s deputies, it’s different from their normal medical training
because the primary goal is to give police
officers the training necessary to sustain
themselves or others in situations with lifethreatening medical emergencies.
Along with the training, a special emergency response equipment kit was developed and issued to all deputies after they
completed the training. The law enforcement individual first aid kit (IFAK) was
assembled to include essential supplies and
devices necessary to combat the three most
common causes of preventable traumatic
death, namely 1) hemorrhage in accessible
and controllable regions; 2) hemorrhage in
inaccessible or uncontrollable areas and 3)
airway/respiratory management.
Photo Courtesy David Kleinman
An officer responding to a scene that’s unsafe for EMS can use a compact kit equipped with the essentials of hemorrhage control and airway management.
A tourniquet could mean the difference between life and death for an officer pinned down by fire.
Officer safety and tactical considerations
are incorporated into every aspect of the
First Five Minutes lesson plan. Officers are
reminded that they’re police officers first
and medical providers second. The program introduction relates the importance
of providing immediate medical care to
the downed officer. The Fort Hood (Texas)
Police Department shooting and the murder of Phoenix Police Department Officer
Travis Murphy illustrate this issue.
At numerous points during the class,
instructors emphasize that this program isn’t designed to be a first aid class,
but rather a survival class for police officers. A law enforcement IFAK is issued to
each student at the beginning of the class
so become familiar with its contents to
ensure rapid retrieval of essential items
when necessary.
Although the IFAK is designed primarily
for law enforcement professionals to treat
fellow officers, deputies are told to use their
discretion at emergency scenes. They’re
encouraged to use their IFAKs, once the
scene is secure, to stabilize civilians when
they feel it can be life-saving in advance of
EMS arrival. Such was the case at the Safeway/Giffords MCI scene.
Because the assisting officer is often the
first person to contact the injured person,
the training stresses the idea that the officer’s
observations and findings are the most significant issues in long-term care and recovery
www.jems.com
MAY 2012
JEMS
43
44. Beyond the Tape
continued from page 43
of the wounded person. Officers are told to
report the following to EMS providers:
T he nature of the injury;
atient’s mental status, including any
P
changes in mental status;
irway control necessary, rates of
A
breathing and circulation;
njuries they saw, who they treated,
I
and how they treated those injuries;
and
A ny unusual findings or concerns.
At the conclusion of the training, the
officers’ skills are evaluated through participation in multiple scenarios. Two evaluators are used for each scenario: one
evaluates officer safety, use of cover and
concealment, tactical movement and other
skills related to police work; the second (an
EMT or paramedic) evaluates the medical
triage and care provided to the patient.
Other Programs
Similar emergency medical training programs address this need. This includes the
specialized tactics for operational rescue
and medicine program (STORM), developed by the Georgia Health Sciences University in conjunction with the National
Tactical Officers Association.
The STORM course provides clearly
defined medical strategies, procedures and
The IFAK
rescue techniques to enhance the safety of
law enforcement personnel and the populations they serve. STORM is tailored to five
unique tactical audiences: self aid-buddy
care, operator, paramedic, medical director and commander. Each course consists of
didactics, hands-on skills stations and tactical scenario-based training.
The Nashville Police Department
recently implemented a modern-day “first
aid” program, which was taught once a
week for five months to their entire roster
of 1,400 active-duty officers. The training
featured lecture and practical skill sessions
training kits, which were issued to each officer as they completed the training program
(see “Partners in Crime,” p. 52–55).
Conclusion
Not all law enforcement agencies consider
emergency care to be part of a police officer’s job. With the ever-increasing call load
and requirements placed on officers, it’s
easy to see how agencies can lessen liability and workload by eliminating a job that’s
already served by fire departments and
EMS agencies.
However, a wounded officer, or an officer responding to a mass casualty incident
well in advance of EMS, presents an opportunity for lives to be saved by law enforcement personnel.
Every officer should have the necessary training and equipment to provide
on-scene emergency medical self care.
They also should be able to assist other
officers and civilians injured during a law
enforcement operation.
Key aspects of implementing a successful
law enforcement emergency care program
are simplicity and ease of use in an emergency. Without those two factors, officers
are limited in what they can effectively do
at a scene.
The training and equipment used by
law enforcement personnel prior to EMS
gaining access to the scene of the Safeway
shooting incident proving it to be worthwhile in a time of crisis, resulting in saved
lives. The First Five Minutes program is
easy to teach, simple to understand and
effective in treating the injured before EMS
arrival. JEMS
David Kleinman, NREMT-P, is a detective with the
Arizona Department of Public Safety and a tactical paramedic with Pima Regional SWAT. com. He can be reached
at 3450drk@comcast.net.
Tammy Kastre, MD, is the medical director for the
Pima County Sheriff’s Department SWAT team and a
board-certified ED physician.
References
1. Sztajnkrycer MD, Callaway DW, Benz AA. Police
officer response to the injured officer: A surveybased analysis of medical care decisions. Prehosp
Disaster Med. 2007;22(4):335–341.
The individual first aid kit includes supplies and
devices necessary to combat the most common
causes of preventable traumatic death.
44
JEMS
MAY 2012
Photo Matthew Strauss
The contents of the IFAK are chosen specifically
for law enforcement officers who would need
to provide care to trauma patients before EMS
arrives on scene. The IFAK’ includes the following items:
A zippered bag with interior elastic straps
for holding contents in place. The exterior of the bag has multiple attachments
points—allowing it to be mounted in
the vehicle, on a backpack or even on a
duty belt.
A pair of trauma shears.
Two emergency compression bandages.
One package of hemostatic combat gauze.
One chest seal.
One tourniquet.
45.
46. Tactical training offers
many benefits to EMS
By William Justice, NREMT-P;
LT. Kerry Massie, NREMT-I;
Jeffrey M. Goodloe, MD, NREMT-P, FACEP
46
JEMS
MAY 2012
47. EMS providers should be prepared to
handle any situation because you never
know when a call could go awry.
Tac Team Alpha: I’ve got visual on
barricaded subject with hostages.
Command: Acknowledge Alpha.
Maintain visual and advise of any
change in behavior or position.
Tac Team Alpha: Subject appears
increasingly disoriented.
Sounds of multiple shots are heard
fired from the subject’s location.
Tac Team Alpha: I’ve got visual on
wounded hostage.
Photos Courtesy OKlahoma highway patrol
Command: Copy Alpha on wounded
hostage.
Command to Tac Team Delta: Go for
entry; go for entry.
Tac Team Delta: Going entry.
Tac Team Delta: Subject secured.
Repeat, subject secured. But officer down! Officer down! Operator
care initiated.
Command: Medics up.
www.jems.com
MAY 2012
JEMS
47
48. Prepared for the Worst
continued from page 47
P
aramedic Tango reaches the downed
officer, finding blood on the ground
next to a large, mid-thigh gunshot wound
in his right leg. The bleeding is already controlled by a tourniquet applied by another
tactical operator involved in the initial team
entry that occurred 65 seconds before Tango
made patient contact. The patient is awake,
alert and complains of thigh pain. He denies
any other injury, and none is found on a
quick but thorough physical exam.
Paramedic Ocean reaches the wounded
hostage at the same time Tango reaches the
downed officer. Ocean finds three gunshot
wounds in the hostage’s chest and abdomen. This patient is awake, talking, anxious
and diaphoretic, and he has an increasingly
rapid radial pulse. Ocean applies an occlusive seal over the largest wound, which is
to the right of the sternum. He finds no exit
wounds during the remainder of his exam,
and he calls for rapid extrication.
A physician and paramedic await the
patients at the tactical command post.
They have vascular access supplies ready
and aeromedical helicopter resources
responding with an estimated arrival time
of five minutes. The wounded law enforcement officer and the wounded hostage
arrive for tactical field care within six minutes of sustaining their wounds.
Troopers practice chest decompressions on a manikin during a training session.
tions. These officers may be dedicated to
full-time service on such teams or accept
these additional roles beyond their daily
police duties. The presence of specialized
operational teams, with specific training,
tasks and capabilities, creates a strong
infrastructure in which to introduce and
advance medical emergency capabilities,
not only within existing teams, but also for
specialized EMS response teams.
Tactical Training
On the day the events described above
occurred, they happened only in training.
But the Oklahoma Highway Patrol (OHP)
EMS Unit state troopers are well aware that
events such as these can occur on any day
at any time.
This knowledge, coupled with a commitment to safety for all Oklahomans,
including their fellow troopers, has guided
OHP leaders in developing an increasingly
sophisticated cadre of all-hazard medical teams for tactical, special event, mass
casualty and natural disaster response
throughout the state. In addition to OHP’s
progressive leadership, many strategically
placed building blocks exist that allow for
law enforcement-related medical emergency success.
Within OHP and other states’ police
organizations, specialized law enforcement teams meet the extraordinary
operational challenges in tactical, riot,
explosive ordinance and disaster situa-
48
JEMS
MAY 2012
Above Beyond
Just like their EMS and fire colleagues,
law enforcement officers are hard-wired
for public service. Within an agency the
size of the OHP, a call for troopers interested in new medical duties will typically
result in a competitive process, yielding
top-flight EMT and paramedic candidates
and graduates.
EMS professionals willing to think outside their usual environments and roles
are often conduits for exciting changes.
Leaders within the University of Oklahoma Department of Emergency Medicine
(OUDEM) were approached by OHP with
hopes of gaining medical oversight support for troopers trained and in training as
EMTs and paramedics.
Select OUDEM physicians and paramedics who expressed interest in participating in the program were screened for
their medical knowledge, law enforcement duty awareness, physical abilities
and teamwork attributes. They were also
required to complete extensive security
background checks. Next came an extensive process that included exhaustive database queries and character references for
each candidate.
After the OHP special team orientation, the selected physicians and paramedics received special “boots on the
ground” training and emergency response
experiences statewide before being
approved to serve on OUDEM’s Special
Operations Medical Oversight and Support (SOMOS) group.
Each physician and paramedic has a formal affiliation with OHP, which provides
them with protection from claims while
they’re on duty in special assignments
and allows for medical liability protection
and worker’s compensation for injuries
through OUDEM.
The physicians and paramedics work
together to ensure coverage is available for
statewide response around the clock, using
response vehicle assets secured under the
Department of Homeland Security funding or responding with a state trooper in a
patrol vehicle.
Specialized Equipment
“High speed/low drag” is the catch-phrase
for expedient, effective operations. Equipment carried on each person and in team
support vehicles is evaluated and imple-