Measurement of Symmetric Dimethylarginine by LC-MS/MS for the Evaluation of Renal Function
•
0 likes•37 views

AACC 2019 -- Symmetric and asymmetric dimethylarginine (SDMA and ADMA) are metabolites of the post-translational modification of arginine residues in histones. SDMA is produced by all body tissues and is cleared almost exclusively by the kidneys, making it an attractive biomarker for the evaluation of renal function. In this study, the development of an LC-MS/MS method for the measurement of SDMA is described and its performance reviewed against traditional renal markers in individuals with microalbuminuria or abnormal thyroid function.

Recommended
More Related Content
Similar to Measurement of Symmetric Dimethylarginine by LC-MS/MS for the Evaluation of Renal Function
Similar to Measurement of Symmetric Dimethylarginine by LC-MS/MS for the Evaluation of Renal Function (20)
More from Covance
More from Covance (20)
Recently uploaded
Recently uploaded (20)
Measurement of Symmetric Dimethylarginine by LC-MS/MS for the Evaluation of Renal Function
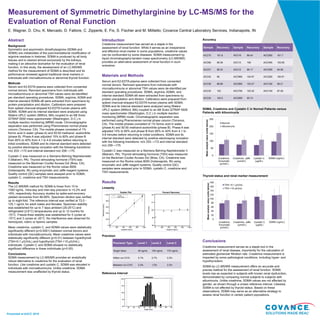
- 1. Presented at AACC 2019 Accuracy SDMA, Creatinine and Cystatin C in Normal Patients versus Patients with Albuminuria Thyroid status and renal marker measurement Conclusions Creatinine measurement serves as a staple tool in the assessment of renal disease, importantly for the calculation of estimated glomerular filtration rate. Creatinine measurement is impacted by some pathological conditions, including hyper- and hypothyroidism. SDMA by LC-MS/MS measurement offers an accurate and precise method for the assessment of renal function. SDMA levels rise as expected in subjects with known renal dysfunction, demonstrated by comparing normal subjects to subjects with albuminuria. Unlike creatinine, SDMA values are not affected by gender, as shown through a unisex reference interval. Likewise, SDMA is not affected by thyroid status. Based on these observations, SDMA may serve as an alternative strategy to assess renal function in certain patient populations. Introduction Creatinine measurement has served as a staple in the assessment of renal function. While it serves as an inexpensive and effective renal marker in some populations, creatinine values can be confounded by some diseases. SDMA measurement by liquid chromatography-tandem mass spectrometry (LC-MS/MS) provides an alternative assessment of renal function in such scenarios. Materials and Methods Serum and K2-EDTA plasma were collected from consented normal donors. Remnant specimens from individuals with microalbuminuria or abnormal TSH values were de-identified per standard operating procedures. SDMA, arginine, ADMA, and internal standard SDMA-d6 were extracted from specimens by protein precipitation and dilution. Calibrators were prepared from spiked charcoal-stripped K2-EDTA human plasma with SDMA. SDMA and its internal standard were analyzed using Waters UPLC system (Milford, MA) coupled to an AB Sciex QTRAP 5500 mass spectrometer (Washington, D.C.) in multiple reaction monitoring (MRM) mode. Chromatographic separation was performed using Phenomenex normal phase column (Torrance, CA). The mobile phases consisted of 1% formic acid in water (phase A) and 50:50 methanol:acetonitrile (phase B). Phase A was adjusted 15% to 60% and phase B from 85% to 40% from 4.1 to 4.8 minutes before returning to initial conditions. SDMA and its internal standard were detected by positive electrospray ionization with the following transitions: m/z 203→172 and internal standard m/z 209→175. Cystatin C was measured on a Siemens Behring Nephelometer II (Malvern, PA). Thyroid stimulating hormone (TSH) was measured on the Beckman Coulter Access DxI (Brea, CA). Creatinine was measured on the Roche cobas 8000 (Indianapolis, IN) using enzymatic and Jaffé reagent systems. Quality control (QC) samples were assayed prior to SDMA, cystatin C, creatinine and TSH measurements. Results Linearity Precision Reference Interval Abstract Background Symmetric and asymmetric dimethylarginine (SDMA and ADMA) are metabolites of the post-translational modification of arginine residues in histones. SDMA is produced by all body tissues and is cleared almost exclusively by the kidneys, making it an attractive biomarker for the evaluation of renal function. In this study, the development of an LC-MS/MS method for the measurement of SDMA is described and its performance reviewed against traditional renal markers in individuals with microalbuminuria or abnormal thyroid function. Methods Serum and K2-EDTA plasma were collected from consented normal donors. Remnant specimens from individuals with microalbuminuria or abnormal TSH values were de-identified per standard operating procedures. SDMA, arginine, ADMA and internal standard SDMA-d6 were extracted from specimens by protein precipitation and dilution. Calibrators were prepared from spiked charcoal-stripped K2-EDTA human plasma with SDMA. SDMA and its internal standard were analyzed using Waters UPLC system (Milford, MA) coupled to an AB Sciex QTRAP 5500 mass spectrometer (Washington, D.C.) in multiple reaction monitoring (MRM) mode. Chromatographic separation was performed using Phenomenex normal phase column (Torrance, CA). The mobile phases consisted of 1% formic acid in water (phase A) and 50:50 methanol: acetonitrile (phase B). Phase A was adjusted 15% to 60% and phase B from 85% to 40% from 4.1 to 4.8 minutes before returning to initial conditions. SDMA and its internal standard were detected by positive electrospray ionization with the following transitions: m/z 203→172 and internal standard m/z 209→175. Cystatin C was measured on a Siemens Behring Nephelometer II (Malvern, PA). Thyroid stimulating hormone (TSH) was measured on the Beckman Coulter Access DxI (Brea, CA). Creatinine was measured on the Roche cobas 8000 (Indianapolis, IN) using enzymatic and Jaffé reagent systems. Quality control (QC) samples were assayed prior to SDMA, cystatin C, creatinine and TSH measurements. Results The LC-MS/MS method for SDMA is linear from 10 to 1000 ng/mL. Intra-day and inter-day precision is <3.2% and <6%, respectively. Accuracy studies by spike-and-recovery yielded recoveries from 89-99%. Specimen dilution was verified up to eight-fold. The reference interval was verified at 73.0 - 125.1 ng/mL for adult males and females. Specimen stability was established for up to 7 days ambient (20-25°C) and refrigerated (2-8°C) temperatures and up to 12 months for -70°C. Freeze-thaw stability was established for 5 cycles at -70°C and 3 cycles at -20°C. No interference was observed for hemolyzed, icteric or lipemic samples. Mean creatinine, cystatin C, and SDMA values were statistically significantly different (p<0.0001) between normal donors and individuals with microalbuminuria. Mean creatinine values were statistically significantly different (p<0.01) between hyperthyroid (TSH<0.1 μIU/mL) and hypothyroid (TSH >10 μIU/mL) individuals. Cystatin C and SDMA showed no statistically significant difference in these individuals (p>0.05). Conclusions SDMA measurement by LC-MS/MS provides an analytically robust alternative to creatinine for the evaluation of renal function. Like creatinine and cystatin C, SDMA was elevated in individuals with microalbuminuria. Unlike creatinine, SDMA measurement was unaffected by thyroid status. Measurement of Symmetric Dimethylarginine by LC-MS/MS for the Evaluation of Renal Function E. Wagner, D. Chu, K. Mercado, D. Fattore, C. Zipperle, E. Fix, S. Fischer and M. Militello; Covance Central Laboratory Services, Indianapolis, IN 0 20 40 60 80 100 120 140 160 180 Creatinine, Enzymatic (μmol/L) Creatinine, Jaffe (μmol/L) Cystatin C (μg/dL) SDMA (ng/mL) Meananalytevalue(unitsbelow) TSH <0.1 μIU/mL TSH >10 μIU/mL 0 50 100 150 200 250 Creatinine, Enzymatic (μmol/L) Creatinine, Jaffe (μmol/L) Cystatin C (μg/dL) SDMA (ng/mL) Meananalytevalue(unitsbelow) Normal Albuminuria Precision Type Level 1 Level 2 Level 3 Target Value 30 ng/mL 150 ng/mL 775 ng/mL Within run CV% 3.1% 2.7% 2.3% Between run CV% 3.3% 1.5% 2.3% Sample Recovery Sample Recovery Sample Recovery ACC75 101.6 ACC18 99.44 ACC565 101.7 ACC66 99.39 ACC15 106 ACC465 102.65 ACC57 96.32 ACC12 99.17 ACC365 94.58 ACC45 98 ACC965 104.97 ACC265 100.91 ACC36 88.89 ACC865 103.27 ACC165 99.21 ACC30 102 ACC765 103.32 ACC140 97.29 ACC24 102.5 ACC665 95.74