Artifacts in Nuclear Medicine with Identifying and resolving artifacts.
2478236.ppt
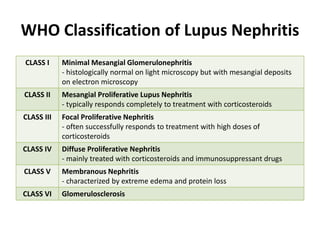
1. WHO Classification of Lupus Nephritis
CLASS I Minimal Mesangial Glomerulonephritis
- histologically normal on light microscopy but with mesangial deposits
on electron microscopy
CLASS II Mesangial Proliferative Lupus Nephritis
- typically responds completely to treatment with corticosteroids
CLASS III Focal Proliferative Nephritis
- often successfully responds to treatment with high doses of
corticosteroids
CLASS IV Diffuse Proliferative Nephritis
- mainly treated with corticosteroids and immunosuppressant drugs
CLASS V Membranous Nephritis
- characterized by extreme edema and protein loss
CLASS VI Glomerulosclerosis
2. International Society of Nephrology/Renal Pathology
Society (INR/RPS) 2003 Classification of Lupus
Nephritis
CLASS I Minimal Mesangial Lupus Nephritis
- normal glomeruli by LM but mesangial immune deposits by IF
CLASS II Mesangial Proliferative Lupus Nephritis
- purely mesangial hypercellularity of any degree or mesangial matrix expansion
by LM, with mesangial immune deposits
- may be a few isolated subepithelial or subendothelial deposits visible by IF or
EM, but not by LM
CLASS III Focal Lupus Nephritis
- active or inactive focal, segmental or global endo- or extracapillary
glomerulonephritis involving <50% of all glomeruli, typically with focal
subendothelial immune deposits, with or without mesangial alterations
III-(A) Active lesions: focal proliferative lupus nephritis
III-(A/C) Active and chronic lesions: focal proliferative and sclerosing lupus
nephritis
III-(C) Chronic inactive lesions with glomerular scars: focal sclerosing lupus
nephritis
(LM – Light Microscopy, IF – Immunofluorescence Microscopy, EM – Electron Microscopy)
Weening et. al. 2004. The Classification of Glomerulonephritis in Systemic Lupus Erythematosus Revisited. J Am Soc Nephrol 15:241-250.
3. International Society of Nephrology/Renal Pathology
Society (INR/RPS) 2003 Classification of Lupus
Nephritis
CLASS IV Diffuse Lupus Nephritis
- active or inactive diffuse, segmental or global endo- or extracapillary glomerulonephritis
involving 50% of all glomeruli, typically with diffuse subendothelial immune deposits, with or
without mesangial alterations
- this class is divided into:
1. diffuse segmental(IV-S) lupus nephritis when 50% of the involved glomeruli have
segmental lesions
2. diffuse global (IV-G) lupus nephritis when 50% of the involved glomeruli have global
lesions
- segmental is defined as a glomerular lesion that involves less than half of the glomerular tuft
- this class includes cases with diffuse wire loop deposits but with little or no glomerular
proliferation
IV-S (A) Active lesions: diffuse segmental proliferative lupus nephritis
IV-G (A) Active lesions: diffuse global proliferative lupus nephritis
IV-S (A/C) Active and chronic lesions: diffuse segmental proliferative and sclerosing
lupus nephritis
Active and chronic lesions: diffuse global proliferative and sclerosing lupus
nephritis
IV-S (C) Chronic inactive lesions with scars: diffuse segmental sclerosing lupus
nephritis
IV-G (C) Chronic inactive lesions with scars: diffuse global sclerosing lupus nephritis
Weening et. al. 2004. The Classification of Glomerulonephritis in Systemic Lupus Erythematosus Revisited. J Am Soc Nephrol 15:241-250.
4. International Society of Nephrology/Renal Pathology
Society (INR/RPS) 2003 Classification of Lupus
Nephritis
CLASS V Membranous Lupus Nephritis
- global or segmental subepithelial immune deposits or their morphologic
sequelae by LM and by IF or EM, with or without mesangial alterations
- may occur in combination with class III or IV in which case both will be
diagnosed
- shows advanced sclerosis
CLASS VI Advanced Sclerosing Lupus Nephritis
- 90% of glomeruli globally sclerosed without residual activity
(LM – Light Microscopy, IF – Immunofluorescence Microscopy, EM – Electron Microscopy)
Weening et. al. 2004. The Classification of Glomerulonephritis in Systemic Lupus Erythematosus Revisited. J Am Soc Nephrol 15:241-250.
5. 3. Enumerate the side-effects of
cyclophosphamide
• Side effects of Cyclophosphamide
– diarrhea
– lethargy
– chemotherapy-induced nausea and vomiting
– bone marrow suppression
– darkening of the skin/nails
– alopecia (hair loss) or thinning of hair
– changes in color and texture of the hair
– hemorrhagic cystitis
Reference: http://www.drugs.com/sfx/cyclophosphamide-side-effects.html
6. 3. Enumerate the side-effects of
cyclophosphamide
• Side effects of Cyclophosphamide
– carcinogenic, potentially causing transitional cell
carcinoma of the bladder as a long-term
complication
– lower the body's immune system
– cause temporary or (rarely) permanent sterility.
Reference: http://www.drugs.com/sfx/cyclophosphamide-side-effects.html
7. Some side effects with cyclophosphamide are potentially
serious and should be reported immediately to a healthcare
provider. These include but are not limited to:
• Signs of an infection, such as chills or a fever
• Blood in the stool
• Blood in the urine (which can be a sign of bladder damage)
• Severe mouth sores
• Signs of an allergic reaction, including unexplained rash,
hives, itching, and unexplained swelling.
• Severe nausea, vomiting, or diarrhea
• Decreased urination, which may be a sign of kidney
damage
• Difficulty breathing or water retention, which may be signs
of congestive heart failure
• Any unusual moles, skin sores that do not heal, or unusual
lumps (which can be signs of new tumors or cancers)
Reference: http://www.drugs.com/sfx/cyclophosphamide-side-effects.html
9. TB of Bones and Joints
• Weight-bearing joints
– spine 40%
– hips 13%
– knees 10%ff
• Phemister’s Triad
– Juxta-articular osteoporosis
– Peripherally located osseous erosions
– Gradual narrowing of the intra-osseous space
Reference: Fauci. Braunwald. Kasper. Hauser. Longo. Jameson. Loscalzo. 2008. Harrison’s Principles of
Internal Medicine, 17th Edition. McGraw-Hill. USA
10. Pott’s Disease (Tuberculous Spondylitis)
• most dangerous form of musculoskeletal TB
– bone destruction, deformity, and paraplegia
• Progressive bone destruction, >2 adjacent
vertebral bodies
– leads to vertebral collapse and kyphosis (due to
collapse in anterior spine)
• Spinal canal narrowing: abscesses, granulation
tissue or direct dural invasion
– leading to SC compression and neurologic deficits
Reference: Fauci. Braunwald. Kasper. Hauser. Longo. Jameson. Loscalzo. 2008. Harrison’s Principles of
Internal Medicine, 17th Edition. McGraw-Hill. USA
11. Clinical Manifestations
• Back pain, stiffness
– thoracic and lumbosacral region most common
• Constitutional symptoms = fever, weight loss
• Most deadly complication = paraplegia
– due to abscess compressing the spinal cord
Reference: Fauci. Braunwald. Kasper. Hauser. Longo. Jameson. Loscalzo. 2008. Harrison’s Principles of
Internal Medicine, 17th Edition. McGraw-Hill. USA
12. Radiographic Findings
• Lytic destruction of
anterior portion of
vertebral body
• Increased anterior
wedging
• Collapse of vertebral
body
Reference: Emedicine. 2009. Pott’s Disease. Retrieved February 16, 2010 from
http://emedicine.medscape.com/article/226141-overview
13. CT Scan
– provides better bony detail of irregular lytic
lesions, sclerosis, disk collapse and disruption of
bone circumference
– reveals early lesions and is more effective for
defining the shape and calcification of soft-tissue
abscesses.
Reference: Emedicine. 2009. Pott’s Disease. Retrieved February 16, 2010 from
http://emedicine.medscape.com/article/226141-overview
14. Radiographic Manifestation
CT scan demonstrating destruction of the right pedicle of T10 due to Pott's disease
Reference: Fauci. Braunwald. Kasper. Hauser. Longo. Jameson. Loscalzo. 2008. Harrison’s Principles of
Internal Medicine, 17th Edition. McGraw-Hill. USA
15. Tuberculosis of Hip and Knee Joints
• Unrecognized joint destruction
• Hip joints
– Involves the head of the femur (common)
– Painful
• Knee joints
– Pain and swelling
• Diagnosis: biopsy, tissue culture and synovial
fluid exam (thick in appearance, high protein
concentration and variable cell count)
Reference: Fauci. Braunwald. Kasper. Hauser. Longo. Jameson. Loscalzo. 2008. Harrison’s Principles of
Internal Medicine, 17th Edition. McGraw-Hill. USA
16. Tuberculosis of the Hip
Lesion on femoral head and acetabulum
Kissing Lesion: hallmark of TB infection
Reference: Singh, Arun Pal. 2009. X-Ray of TB of Hip Joint. Retrieved February 16, 2010 from
http://boneandspine.com/muculoskeletal-radiology/xray-of-tuberculosis-of-hip-joint/
17. calcified debris in the supra-patellar bursa
Reference: Palmer & Reeder. 2009. The Imaging of Tropical Diseases. Retrieved February 16, 2010 from
http://www.isradiology.org/tropical_deseases/tmcr/chapter5/lymphadenopathy.htm
19. Clinical Manifestations
• Local symptoms predominate
• Up to one third of patients may concomitantly
have pulmonary manifestations
• Common symptoms include:
– Urinary frequency
– Dysuria
– Nocturia
– Hematuria
– Abdominal and Flank pain
Harrison’s Principle of Internal Medicine, 17th ed. P1011-1012
20. Clinical Manifestations
• In females:
– May affect the fallopian tubes and the
endometrium causing infertility, pelvic pain and
menstrual abnormalities
• In males:
– Primarily affects the epididymis, producing a slight
tender mass that may drain externally through a
fistulous tract; orchitis and prostatitis.
Harrison’s Principle of Internal Medicine, 17th ed. P1011-1012
21. Laboratory Manifestations
• Urinalysis:
– Pyuria and Hematuria
• Urine Culture:
– Pyuria but negative for common organisms
causing UTI
– Culture of three morning urine specimens positive
for Mycobacterium tuberculosis is a definitive
diagnosis.
Harrison’s Principle of Internal Medicine, 17th ed. P1011-1012
22. Radiographic Manifestations
• Intravenous pyelography
• Abdominal CT
• MRI
Deformities, obstructions, calcifications and ureteral
strictures are suggestive findings in genitourinary
tuberculosis.
Harrison’s Principle of Internal Medicine, 17th ed. P1011-1012
24. Isoniazid
• Isoniazid-induced hepatitis-most common major
toxic effect
• Peripheral neuropathy
• CNS toxicity-memory loss, psychosis,seizures
• Fever and skin rashes
• Drug-induced SLE
• Hematologic abnormalities
• Provocation of pyridoxine deficiency anemia
• Tinnitus
• Gastrointestinal discomfort
Katzung, B, Basic and Clinical Pharmacology 10th ed., McGraw Hill 2007, page 773
25. Rifampicin
• Orange urine, sweat and tears
• Rashes
• Thrombocytopenia
• Nephritis
• Light-chain proteinuria
• Flu-like sydrome(fever, chills, myalgia, anemia
and thrombocytopenia)
Katzung, B, Basic and Clinical Pharmacology 10th ed., McGraw Hill 2007, page 774
26. Ethambutol
• Retrobulbar neuritis
most common serious adverse event
Loss of visual acuity and red-green color blindness
• Hypersensitivity syndrome consisting of
cutaneous reaction (such as rash or exfoliative
dermatitis)
• Fever and lymphadenopathy
http://www.drugs.com/sfx/ethambutol-side-effects.html
Katzung, B, Basic and Clinical Pharmacology 10th ed., McGraw Hill 2007, page 774
28. Anti-TB regimen in special situations of liver
disease, renal impairment, and pregnancy.
29. Liver disease
• Patients with pre-existing liver disease can receive the usual TB
regimens provided that there is no clinical evidence of chronic liver
disease, hepatitis virus carriage, a past history of acute hepatitis,
current excessive alcohol consumption.
• However, hepatotoxic reactions to anti-TB drugs may be more
common among these patients and should therefore be anticipated
• The first-line drugs HRZ are all associated with hepatotoxicity.
– Pyrazinamide is the most hepatotoxic
Treatment of tuberculosis: guidelines - 4th ed. WHO
http://whqlibdoc.who.int/publications/2010/9789241547833_eng.pdf
30. • The more unstable or severe the liver disease is, the fewer
hepatotoxic drugs should be used.
• In general, patients with chronic liver disease should not receive
pyrazinamide. All other drugs can be used, but close monitoring
of liver enzymes is advised.
If the serum AST level is more than 3 times normal before the initiation of
treatment, the following regimens should be considered .
• Two hepatotoxic drugs (rather than the three in the standard regimen):
9 months of HRE
2 months of HRSE followed by 6 months of HR
6–9 months of RZE.
• One hepatotoxic drug:
2 months of HES, followed by 10 months of HE
• No hepatotoxic drugs:
18–24 months of streptomycin, ethambutol and a fluoroquinolone.
31. Renal impairment
• The recommended initial TB treatment regimen for patients with
renal failure or severe renal insufficiency is 2 months of HRZE,
followed by 4 months of HR.
• Isoniazid and rifampicin are eliminated by biliary excretion, so no
change in dosing is necessary.
• There is significant renal excretion of ethambutol and metabolites
of pyrazinamide and doses should therefore be adjusted.
• Three times per week administration of these two drugs at the
following doses is recommended: pyrazinamide (25 mg/kg), and
ethambutol (15 mg/kg)
Treatment of tuberculosis: guidelines - 4th ed. WHO
http://whqlibdoc.who.int/publications/2010/9789241547833_eng.pdf
32. Renal impairment
• While receiving isoniazid, patients with severe renal insufficiency or
failure should also be given pyridoxine in order to prevent
peripheral neuropathy.
• Streptomycin should be avoided in patients with renal failure
because of an increased risk of nephrotoxicity and ototoxicity.
• If streptomycin must be used, the dosage is 15 mg/kg, two or three
times per week, to a maximum of 1 gram per dose, and serum
levels of the drug should be monitored.
33. Pregnancy
• Women of childbearing age should be asked about current or
planned pregnancy before starting TB treatment.
• A pregnant woman should be advised that successful treatment of
TB with the standard regimen is important for successful outcome
of pregnancy.
• With the exception of streptomycin, the first line anti-TB drugs are
safe for use in pregnancy
– streptomycin is ototoxic to the fetus and should not be used during
pregnancy.
• Pyridoxine supplementation is recommended for all pregnant
women taking isoniazid
Treatment of tuberculosis: guidelines - 4th ed. WHO
http://whqlibdoc.who.int/publications/2010/9789241547833_eng.pdf
Editor's Notes
Hemorrhagic cystitis is a frequent complication, but this is prevented by adequate fluid intake and Mesna (sodium 2-mercaptoethane sulfonate). Mesna is a sulfhydryl donor and binds acrolein.
In the United States, tuberculosis of the bones and joints is responsible for ~10% of extrapulmonary cases. In bone and joint disease, pathogenesis is related to reactivation of hematogenous foci or to spread from adjacent paravertebral lymph nodes.
While the upper thoracic spine is the most common site of spinal tuberculosis in children, the lower thoracic and upper lumbar vertebrae are usually affected in adults.
femoral head has disappeared, the acetabulum is irregular and sclerotic, and there are cystic changes both in the femoral neck and around the joint.
A healed but badly damaged joint, with partial destruction of the upper end of the tibia, and a lot of new bone and loose fragments. There is calcified debris in the supra-patellar bursa.