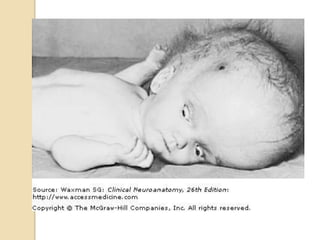
9. Congenital/infantile
hydrocephalus
The cranial bones fuse by the end of
the third year; for the head to enlarge,
hydrocephalus must develop before
this time.
It may begin in utero but usually
happens in the first few months of life
10. even of mild degree, it molds the
shape of the skull in early life
in radiographs the inner table is
unevenly thinned, an appearance
referred to as "beaten silver" or as
convolutional or digital markings.
The frontal regions are unusually
prominent [bossing]
11. Face relatively small and pinched
Skin over the cranial bones tight and
thin
Prominent distended veins.
12. Usual causes
Intraventricular matrix hemorrhages in
premature infants
fetal and neonatal infections
Arnold -Chiari malformation
Aqueductal atresia and stenosis
Dandy-Walker syndrome.
13. Clinical features
Rapid head enlargement
Tense anterior and posterior
fontanelles
Infant is fretful, feeds poorly, and may
vomit frequently.
With continued enlargement of the
brain, inactivity sets in and the infant
appears languid, uninterested in his
surroundings, and unable to sustain
activity.
14. Later, the upper eyelids are retracted
and the eyes tend to turn down
paralysis of upward gaze
sclerae above the irises are visible;
"setting-sun sign"
caused by hydrocephalic pressure on
the mesencephalic tegmentum.
15. Gradually the infant adopts a posture
of flexed arms and flexed or extended
legs.
Signs of corticospinal tract damage
are usually elicitable.
Movements are feeble and sometimes
the arms show tremors
16. later the optic discs become pale and
vision is reduced.
If the hydrocephalus becomes
arrested, the infant or child is retarded
but often surprisingly verbal.
The head may be so large that the
child cannot hold it up and must
remain in bed
17. If the head is only moderately
enlarged, the child may be able to sit
but not stand or stand but not walk.
If ambulatory, the child is clumsy.
Acute exacerbations of hydrocephalus
or a febrile illness may cause
vomiting, stupor, or coma.
22. Intracranial pressure
The intact cranium and vertebral
canal, together with the relatively
inelastic dura, form a rigid container,
such that an increase of any of its
contents—brain, blood, or CSF—will
elevate the ICP.
23. an increase in volume of any one of
these three components must be at
the expense of the other two [Monro-
Kellie doctrine]
Compensatory measures
Small increments in brain volume do
not immediately raise the ICP due to
displacement of CSF from the cranial
cavity into the spinal canal
24. deformation of the brain and limited
stretching of dural folds, specifically,
the falx cerebri and the tentorium
cerebelli
Failure of compensating measures -
mass within one dural compartment
leads to displacement, or "herniation"
from that compartment into an
adjacent one
25. Further increment in brain volume will
reduce the volume of intracranial
blood contained in the veins and dural
sinuses.
CSF is formed more slowly
As the brain, blood, or CSF volumes
continue to increase, the
accommodative mechanisms fail and
ICP rises exponentially
26. Cerebral perfusion pressure
(CPP).
numerical difference between ICP and
mean blood pressure within the
cerebral vessels
elevation in ICP that approaches the
level of mean systemic blood
pressure→ widespread reduction in
cerebral blood flow/perfusion.
27. In its most severe form, this global
ischemia produces brain death.
Lesser degrees of raised ICP and
reduced cerebral circulation cause
correspondingly less severe, but still
widespread, cerebral infarction that is
similar to what arises after cardiac
arrest.
28. Determinants of the degree of cerebral
damage are the severity and the
duration of reduction of CPP
29. CAUSES OF RAISED ICP
A cerebral or extracerebral mass
such as brain tumor; massive
infarction with edema; extensive
traumatic contusion; parenchymal,
subdural, or extradural hematoma; or
abscess
Generalized brain swelling, as
occurs in ischemic–anoxic states,
acute hepatic failure, hypertensive
encephalopathy, hypercarbia, and the
Reye hepatocerebral syndrome
30. An increase in venous pressure-
cerebral venous sinus thrombosis,
heart failure, or obstruction of the
superior mediastinal or jugular veins.
Obstruction to the flow and
absorption of CSF - within the
ventricles or in the subarachnoid
space at the base of the brain,
extensive meningeal disease
31. Any process that expands the
volume of CSF (meningitis,
subarachnoid hemorrhage) or
increases CSF production (choroid
plexus tumor).
32. CLINICAL FEATURES OF
RAISED ICP
Headache
Nausea and vomiting
Drowsiness
Ocular palsies
Papilledema →periodic visual
obscurations.
Protracted papilledema →optic
atrophy and blindness
33. The consequences of increased
intracranial pressure differ in
infants and small children, whose
cranial sutures have not closed.
34. TRANSTENTORIAL AND
OTHER HERNIATIONS
An expanding lesion in the
supratentorial compartment, such as a
subdural hematoma or a tumor in a
cerebral hemisphere, may push the
medial part of the temporal lobe (the
uncus) down into the tentorial notch
35. UNCAL herniation
presses on the ipsilateral oculomotor
nerve.
The first clinical sign of this event is
impairment of the pupillary light reflex
because the preganglionic
parasympathetic fibers for constriction
of the pupil are superficially located in
the nerve.
36. Further herniation
damage to descending motor fibers in
one or both cerebral peduncles →
weakness, spasticity, and exaggerated
tendon reflexes on either side or
bilaterally.
midbrain displacement toward the
opposite side→the pressure of the rigid
edge of the tentorium on the basis
pedunculi →upper motor neuron
paresis on the same side of the body as
the cerebral lesion.
37. Sometimes the downward
displacement of the brain →occlusion
of one or both posterior cerebral
arteries by stretching these vessels
over the free edge of the tentorium,
38. Later stages
Contralateral oculomotor nerve may
be affected.
The pupil that dilates first is the most
reliable lateralizing sign for the
causative lesion.
39. Subfalcial herniation
A space-occupying lesion pushes the
cingulate gyrus of one hemisphere
across the midline beneath the
anterior part of the free edge of the
falx cerebri.
40. Upward transtentorial herniation
brain stem and cerebellum are
displaced into the supratentorial
compartment by a mass in the
posterior fossa.
may also cause medullary coning,
when the brain stem and part of the
cerebellum descend through the
foramen magnum into the spinal
canal.
41. Cerbellar tonsils compress the
medulla, and the condition can be
quickly fatal.
Medullary coning can occur after
withdrawal of CSF from the lumbar
subarachnoid space in a patient with
raised intracranial pressure
42.
43.
44.
45.
46.
47.
48.
49.
50. (1) cingulate herniation under the falx, (2) downward
transtentorial (central) herniation, (3) uncal herniation over the
edge of the tentorium, or (4) cerebellar tonsillar herniation into
the foramen magnum. Coma and ultimately death result when
(2), (3), or (4) produces brainstem compression.