Anatomy of the Male internal genitalia.pptx
•Download as PPTX, PDF•
0 likes•84 views

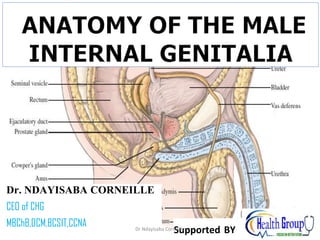
Include: the testes, the epididymis, the vas deferens, the seminal vesicles, the prostate gland, and the Cowper’s glands. The testes, (To Testify) the paired, oval-shaped organs that produce sperm and male sex hormones, are located in the scrotum. They are highly innervated and sensitive to touch and pressure. The testes produce testosterone, which is responsible for the development of male sexual characteristics and sex drive (libido).

Recommended
More Related Content
Similar to Anatomy of the Male internal genitalia.pptx
Similar to Anatomy of the Male internal genitalia.pptx (20)
More from Dr Ndayisaba Corneille
More from Dr Ndayisaba Corneille (20)
Recently uploaded
Recently uploaded (20)
Anatomy of the Male internal genitalia.pptx
- 1. Dr. NDAYISABA CORNEILLE CEO of CHG MBChB,DCM,BCSIT,CCNA Supported BY Dr Ndayisaba Corneille 1
- 2. Contents Vas Deferens Seminal vesicles Ejaculatory Ducts Prostate Clinical notes Dr Ndayisaba Corneille 2
- 3. Internal Male Sexual Organs • Include: • the testes, the epididymis, the vas deferens, the seminal vesicles, the prostate gland, and the Cowper’s glands. • The testes, (To Testify) the paired, oval-shaped organs that produce sperm and male sex hormones, are located in the scrotum. • They are highly innervated and sensitive to touch and pressure. • The testes produce testosterone, which is responsible for the development of male sexual characteristics and sex drive (libido). Dr Ndayisaba Corneille 3
- 5. Ejaculatory Duct • Ejaculatory duct ejects semen and sperm into the urethra • Formed from the fusion of terminal portion of the ductus deferens and the duct of the seminal vesicles Dr Ndayisaba Corneille 5
- 6. Ejaculatory Ducts • The two ejaculatory ducts are each less than 1 inch (2.5 cm) long and are formed by the union of the vas deferens and the duct of the seminal vesicle • The ejaculatory ducts pierce the posterior surface of the prostate and open into the prostatic part of the urethra, close to the margins of the prostatic utricle; their function is to drain the seminal fluid into the prostatic urethra. Dr Ndayisaba Corneille 6
- 7. Vas Deferens • Is a thick-walled tube about 18 inches (45 cm) long that conveys mature sperm from the epididymis to the ejaculatory duct and the urethra. • Arises from the lower end or tail of the epididymis and passes through the inguinal canal. It emerges from the deep inguinal ring and passes around the lateral margin of the inferior epigastric artery Dr Ndayisaba Corneille 7
- 8. Contd • Passes downward and backward on the lateral wall of the pelvis and crosses the ureter in the region of the ischial spine. • Runs medially and downward on the posterior surface of the bladder • Its terminal part is dilated to form the ampulla . The inferior end of the ampulla narrows down and joins the duct of the seminal vesicle to form the ejaculatory duct. Dr Ndayisaba Corneille 8
- 10. Dr Ndayisaba Corneille 10
- 11. SEMINAL VESICLES • Are two lobulated organs about 2 inches. (5 cm) long lying on the posterior surface of the bladder • On the medial side of each vesicle lies the terminal part of the vas deferens. • Posteriorly, the seminal vesicles are related to the rectum. • Inferiorly, each seminal vesicle narrows and joins the vas deferens of the same side to form the ejaculatory duct. • Each seminal vesicle consists of a much-coiled tube embedded in connective tissue. Dr Ndayisaba Corneille 11
- 12. Blood Supply Arteries • The inferior vesicle and middle rectal arteries. Veins • The veins drain into the internal iliac veins. Lymph Drainage • The internal iliac nodes. Dr Ndayisaba Corneille 12
- 13. Function • The function of the seminal vesicles is to produce a secretion that is added to the seminal fluid. • The secretions nourish the spermatozoa. • During ejaculation the seminal vesicles contract and expel their contents into the ejaculatory ducts, thus washing the spermatozoa out of the urethra. Dr Ndayisaba Corneille 13
- 14. Accessory Structures • Bulbourethral glands - produces fluid that lubricates penis and neutralizes urinary acids; located at the base of the penis –Cowper’s gland • Semen - composed of 60% seminal vesicle fluid, 30% prostatic fluid, 10 % sperm and various secretions Dr Ndayisaba Corneille 14
- 15. Semen • The whitish fluid expelled through the opening of the penis (urethra) during ejaculation. • Most of the ejaculate is made up of the fluid that supports the sperm. • Besides sperm, (1%) semen is made up of fluids; 65% from the seminal vesicles, 30 to 35% from the prostate and 5% from the vasa. • The amount of ejaculate you produce can vary, from just a few drops to about a teaspoon full (2 to 6 ml). • One amount of ejaculate may contain between 40 million to 600 million sperm depending on the volume and the length of time stored before ejaculating. • Yet, the quantity of sperm produced will only cover the head of a pin. Dr Ndayisaba Corneille 15
- 16. Journey of the Sperm interstitial cells- testosterone
- 17. Journey of the Sperm sperm production in the seminferous tubules
- 18. Journey of the Sperm sperm storage in the epididymis
- 19. Journey of the Sperm transport in the vas deferens
- 20. Journey of the Sperm ampulla - storage
- 21. Journey of the Sperm fluid from the seminal vessicles ejaculatory duct
- 22. Journey of the Sperm fluid from the prostate gland
- 23. Journey of the Sperm cowper’s gland
- 24. Journey of the Sperm ejaculation
- 25. Erectile and Ejaculatory Abnormalities Peyronie’s disease: • An abnormal condition characterized by an excessive curvature of the penis that can make erection quite painful • Etiology: buildup of fibrous tissue in the penile shaft. • It usually requires medical attention. Dr Ndayisaba Corneille 25
- 26. Phimosis • Phimosis is a medical condition in which the foreskin of the penis of an uncircumcised male cannot be fully retracted. • The word derives from the Greek phimos ("muzzle"). • In the United States, circumcision is the surgical treatment of choice for correction of phimosis Dr Ndayisaba Corneille 26
- 27. Retrograde ejaculation: • Ejaculation in which the ejaculate empties into the bladder. • The external sphincter remains closed preventing the expulsion of the seminal fluid; the internal sphincter remains open allowing the ejaculate to empty into the bladder. • The result is a dry orgasm. • Etiology: possible (earlier types of ) prostate surgery, tranquilizers, illness, and accidents. • Harmless discharged with urine. • Infertility may be the result. Dr Ndayisaba Corneille 27
- 28. Priapism: • Painful erections that persist for hours or days. • Etiology: mechanisms that drain the blood that erects the penis are damaged and so cannot return the blood to the circulatory system. • Caused by the following medical conditions: leukemia, sickle cell anemia, or diseases of the spinal cord. • Treatment: may become a medical emergency, since prolonged erections beyond six hours can starve the penile tissues of oxygen, leading to permanent tissue deterioration. • Surgery or drugs are sometimes used. Dr Ndayisaba Corneille 28
- 29. Prostate • Location and Description • It is a fibromuscular glandular organ that surrounds the prostatic urethra • It is about 1.25 inches (3 cm) long and lies between the neck of the bladder above and the urogenital diaphragm below • The prostate is surrounded by a fibrous capsule • It has a somewhat conical shape and has a base, which lies against the bladder neck above, and an apex, which lies against the urogenital diaphragm below. • The two ejaculatory ducts pierce the upper part of the posterior surface of the prostate to open into the prostatic urethra at the lateral margins of the prostatic utricle Dr Ndayisaba Corneille 29
- 30. Prostate in coronal section (A), sagittal section (B), and horizontal section (C). In the coronal section, note the openings of the ejaculatory ducts on the margin of the prostatic utricle Dr Ndayisaba Corneille 30
- 31. Relations • Superiorly: The base of the prostate is continuous with the neck of the bladder, the smooth muscle passing without interruption from one organ to the other. The urethra enters the center of the base of the prostate. Dr Ndayisaba Corneille 31
- 32. Contd • Inferiorly: The apex of the prostate lies on the upper surface of the urogenital diaphragm. The urethra leaves the prostate just above the apex on the anterior surface Dr Ndayisaba Corneille 32
- 33. Contd • Anteriorly: The prostate is related to the symphysis pubis, separated from it by the extraperitoneal fat in the retropubic space (cave of Retzius). The prostate is connected to the posterior aspect of the pubic bones by the fascial puboprostatic ligaments Dr Ndayisaba Corneille 33
- 34. Contd • Posteriorly: The prostate is closely related to the anterior surface of the rectal ampulla and is separated from it by the rectovesical septum (fascia of Denonvilliers). This septum is formed in fetal life by the fusion of the walls of the lower end of the rectovesical pouch of peritoneum, which originally extended down to the perineal body. Dr Ndayisaba Corneille 34
- 35. Contd • Laterally: The prostate is embraced by the anterior fibers of the levator ani as they run posteriorly from the pubis Dr Ndayisaba Corneille 35
- 36. Structure the Prostate • The numerous glands of the prostate are embedded in a mixture of smooth muscle and connective tissue, and their ducts open into the prostatic urethra. • The prostate is incompletely divided into five lobes The anterior lobe lies in front of the urethra and is devoid of glandular tissue. Dr Ndayisaba Corneille 36
- 37. Contd • The median, or middle, lobe is the wedge of gland situated between the urethra and the ejaculatory ducts. Its upper surface is related to the trigone of the bladder; it is rich in glands. Dr Ndayisaba Corneille 37
- 38. Contd • The posterior lobe is situated behind the urethra and below the ejaculatory ducts and also contains glandular tissue. The right and left lateral lobes lie on either side of the urethra and are separated from one another by a shallow vertical groove on the posterior surface of the prostate. The lateral lobes contain many glands. Dr Ndayisaba Corneille 38
- 39. PROSTATE LOBES • Inferioposterior lobe – it lies to the posterior to the urethra and inferior to the ejaculatory duct • Inferiolateral lobe- it lies directly to the urethra • Superiomedial lobe- inferior to the ejaculatory duct • Anteriomedial lobe- lateral to the prostatic urethra Dr Ndayisaba Corneille 39
- 40. Function of the Prostate • The prostate produces a thin, milky fluid containing citric acid and acid phosphatase that is added to the seminal fluid at the time of ejaculation. • The smooth muscle, which surrounds the glands, squeezes the secretion into the prostatic urethra. The prostatic secretion is alkaline and helps neutralize the acidity in the vagina. Dr Ndayisaba Corneille 40
- 41. Blood Supply • Arteries • Branches of the inferior vesical and middle rectal arteries. • Veins • The veins form the prostatic venous plexus, which lies outside the capsule of the prostate . The prostatic plexus receives the deep dorsal vein of the penis and numerous vesical veins and drains into the internal iliac veins. • . Dr Ndayisaba Corneille 41
- 42. • Lymph Drainage Internal iliac nodes. • Nerve Supply Inferior hypogastric plexuses. The sympathetic nerves stimulate the smooth muscle of the prostate during ejaculation Dr Ndayisaba Corneille 42
- 43. Dr Ndayisaba Corneille 43
- 44. Prostate Cancer The Facts* • About 70% of all diagnosed cancers: men aged 65 years or older. Over the past 20 years, the survival rate increased from 67% to 97%. Studies have found the following risk factors for prostate cancer: • Age: Age is the main risk factor for prostate cancer. This disease is rare in men younger than 45. The chance of getting it goes up sharply as a man gets older. • Family history: A man's risk is higher if there is family history • Race: Prostate cancer is more common in African American • Diet: Some studies suggest that men who eat a diet high in animal fat or meat may be at increased risk for prostate cancer. Screening: • Digital Rectal Exam: The doctor inserts a lubricated, gloved finger into the rectum and feels the prostate through the rectal wall. The prostate is checked for hard or lumpy areas. • Blood test for PSA: A lab checks the level of PSA in a man's blood sample. Prostate cancer may also cause a high PSA level. • The digital rectal exam and PSA test can detect a problem in the prostate. They cannot show whether the problem is cancer or a less serious condition. Dr Ndayisaba Corneille 44
- 45. Symptoms • A man with prostate cancer may not have any symptoms. For men who have symptoms of prostate cancer, common symptoms include: • Urinary problems – Not being able to urinate – Having a hard time starting or stopping the urine flow – Needing to urinate often, especially at night – Weak flow of urine – Urine flow that starts and stops – Pain or burning during urination • Difficulty having an erection • Blood in the urine or semen • Frequent pain in the lower back, hips, or upper thighs • Sometimes symptoms are not due to cancer. Dr Ndayisaba Corneille 45
- 46. Enlarged Prostrate An enlarged prostate means the gland has grown bigger. Prostate enlargement happens to almost all men as they get older. As the gland grows, it can press on the urethra and cause urination and bladder Symptoms • Slowed or delayed flow of urine • Weak urine stream • Dribbling after urinating • Straining to urinate • Strong and sudden need to urinate • Incomplete emptying of your bladder • Incontinence • Pain and bloody urine Dr Ndayisaba Corneille 46
- 47. Clinical Notes Prostate Examination • The prostate can be examined clinically by palpation by performing a rectal examination. • The examiner's gloved finger can feel the posterior surface of the prostate through the anterior rectal wall. Dr Ndayisaba Corneille 47
- 48. Prostate Activity and Disease • It has been shown that trace amounts of proteins produced specifically by prostatic epithelial cells are found in peripheral blood. • In certain prostatic diseases, notably cancer of the prostate, these proteins appear in the blood in increased amounts. • The specific protein level can be measured by a simple laboratory test called the PSA (prostate-specific antigen) test. Dr Ndayisaba Corneille 48
- 49. Benign Enlargement of the Prostate (BPH) • Benign enlargement of the prostate is common in men older than 50 years. • The median lobe of the gland enlarges upward and encroaches within the sphincter vesicae, located at the neck of the bladder. • The leakage of urine into the prostatic urethra causes an intense reflex desire to micturate. • The patient experiences difficulty in passing urine and the stream is weak. • Back-pressure effects on the ureters and both kidneys are a common complication. Dr Ndayisaba Corneille 49
- 50. Dr Ndayisaba Corneille 50
- 51. END END THANKS FOR LISTENING By DR NDAYISABA CORNEILLE MBChB,DCM,BCSIT,CCNA Contact us: amentalhealths@gmail.com/ ndayicoll@gmail.com whatsaps :+256772497591 /+250788958241 Dr Ndayisaba Corneille 51