Rapid Detection of MDR-TB Using Molecular Methods
•
0 likes•312 views

This document discusses rapid detection of multi drug resistant tuberculosis (MDR-TB). It begins with an introduction to tuberculosis, including prevalence, causative bacteria, types of infection, and emergence of MDR-TB. It then describes the molecular mechanisms of rifampicin and isoniazid resistance. The objectives are to rapidly detect tuberculosis using molecular methods like line probe assay and GeneXpert. The results found both tests had 99% sensitivity and 100% specificity. The conclusions state these tests provide results within hours, allowing faster treatment compared to conventional methods.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Rapid Detection of MDR-TB Using Molecular Methods
Similar to Rapid Detection of MDR-TB Using Molecular Methods (20)
More from Mayur D. Chauhan
More from Mayur D. Chauhan (20)
Recently uploaded
Recently uploaded (20)
Rapid Detection of MDR-TB Using Molecular Methods
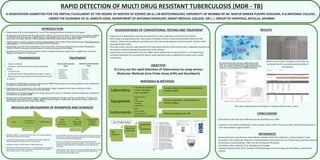
- 1. RAPID DETECTION OF MULTI DRUG RESISTANT TUBERCULOSIS (MDR - TB) A DISSERTATION SUBMITTED FOR THE PARTIAL FULFILLMENT OF THE DEGREE OF MASTER OF SCIENCE (M.Sc.) IN BIOTECHNOLOGY, UNIVERSITY OF MUMBAI BY Mr. MAYUR DINKAR PUSHPA CHAUHAN, R.D.NATIONAL COLLEGE, . UNDER THE GUIDANCE OF Dr. AMEETA JOSHI, DEPARTMENT OF MYCOBACTERIOLOGY, GRANT MEDICAL COLLEGE, SIR J. J. GROUP OF HOSPITALS, BYCULLA, MUMBAI INTRODUCTION Ÿ Tuberculosis (TB or Consump on) is one of the leading bacterial infec ons in the world. Ÿ According to the World Health Organiza on (WHO), around one-third of the world's popula on (>40%) is infected with this disease. Tuberculosis is responsible for more than 2 million deaths and 8 million new cases annually. Nearly 2 billion people have latent tuberculosis infec on (LTBI). Ÿ Tuberculosis is mainly caused by bacteria belonging to the family of Mycobacteriaceae. Mycobacterium tuberculosis is the key bacteria causing fatal TB in Humans. Ÿ Depending upon the site of infec on, TB can be either Pulmonary (Restricted to Lower Respiratory Tract) or Extra-Pulmonary (Dissemina on to other vital parts of the Body) Ÿ Symptoms of Pulmonary tuberculosis mainly include produc ve cough, fever, weight loss, anorexia, fa gue, hemoptysis or chest pain. Ÿ Emergence of Mul drug-resistant tuberculosis (MDR-TB) has posed a serious problem and is defined as resistance to Rifampicin and Isoniazid. Ÿ Development of resistance to the an -tubercular drugs in pa ents who have no history of an - tubercular treatment is termed as Primary MDR. Ÿ Emergence of resistance against the drugs during the course of infec on and an -tubercular treatment is termed as Secondary MDR. Ÿ Resistance to an -tubercular drugs is caused by inadequate dosage, wrong combina on of drugs and inadequate treatment of the pa ent. MDR-TB takes longer to treat with second-line drugs, which are more expensive and have more side-effects. MOLECULAR MECHANISMS OF RIFAMPICIN AND ISONIAZID Ÿ Rifampicin (RMP) is a bactericidal an -tubercular drug belonging to the Rifamycin group of an -bio cs. Ÿ It inhibits the transcrip on of mycobacterial DNA by binding the DNA-dependent RNA polymerase in the cytoplasm. Ÿ rpoB gene codes for the β-subunit of RNA polymerase. Ÿ Muta ons in this gene mainly occurs in the 81 basepairs (26 codons) central region which leads to resistance to RMP. More than 96% of the muta ons occur in this region only. Ÿ Isoniazid (INH) is another first-line an -tubercular drug. Isoniazid is bactericidal to rapidly dividing mycobacteria, but is bacteriosta c if the mycobacteria are slow-growing. Ÿ INH is a pro-drug that is ac vated in the bacterial cell by the mycobacterial enzyme catalase-peroxidase. This enzyme is coded by the gene katG. Muta ons in this gene leads to high level of resistance. Ÿ Another gene, inhA, codes for the enzyme NADH dependent enoyl ACP reductase. This enzyme is involved in the biosynthesis of mycobacterial cell wall fa y acids. DISADVANTAGES OF CONVENTIONAL TESTING AND TREATMENT Ÿ Tuberculosis is detected by culturing the specimens on the Lowenstein and Jensen (LJ) medium. Ÿ MTB, being a slow growing strain, takes about 6-8 weeks of me to show demonstrable colonies on the medium. Biochemical tes ng for specia on was me consuming and gives varied results for species which were gene cally similar. Ÿ Thus there was a need for rapid detec on of tuberculosis infec on which would help in adequate treatment of the pa ents without allowing the progression of the disease. Ÿ Liquid culture was introduced in the year 1980's which reduced the turnaround me to 2-3 weeks. Drug sensi vity tes ng by the conven onal solid or liquid methods took an addi onal 4-6 weeks and 2 weeks respec vely. OBJECTIVE To Carry out the rapid Detec on of Tuberculosis by using various Molecular Methods (Line Probe Assay (LPA) and GeneXpert) Test report obtained from GeneXpert: It indicates that the test is valid. CONCLUSIONS Ÿ Sensi vity of the Tests were 99% whereas the Specificity was 100% Ÿ Superior to Conven onal Methods as they provide results within a few hours which would allow pa ents to start the treatment regimen faster. REFERENCES Ÿ Marinus Barnard, Linda Parsons, Paolo Mio o, Daniella Cirillo, Knut Feldmann, Cris na Gu errez, Akos Somoskovi, 2012, Molecular Detec on of Drug-Resistant Tuberculosis By Line Probe Assay, Laboratory Manual for Resource-Limited Se ngs, FIND, Unit Aid and Expand-TB project Ÿ Soundiram Indira, Cepheid, 2012, GeneXpert Technology. Ÿ Subhash Chandra Parija, 2012, Textbook of Microbiology and Immunology, Second edi on, published by Elsevier RESULTS • Person to Person • Present in Air-borne par cles termed as Droplet Nuclei. • 1-5 µm in size • Generated when infected pa ents cough or sneeze • Bacteria may remain viable in the environment up ll 8 months. TREATMENT First-Line An -tubercular Drugs • Streptomycin • Isoniazid • Rifampicin • Ethambutol • Pyrazinamide Second-Line An -tubercular Drugs • Ciprofloxacin • Cycloserine • Ethionamide • Ofloxacin • Kanamycin • Levofloxacin • Capreomycin TRANSMISSION MATERIALS & METHODS On performing ZN staining, Mtb shows pink rods on a blue background in Oil immersion lens. The smears are then graded based on the number of mycobacteria in different fields. Based on the number of bands on the Strip, we can determine the sensi vity and resis vity of the bacteria.